

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Both Alzheimer pathology and cerebral infarcts are common in older people, making the influence of cerebral infarcts on cognition a matter of interest (1-3). Several magnetic resonance imaging (MRI)-based studies have documented that silent or symptomatic infarcts are associated with poorer cognitive performance, cognitive decline, or increased likelihood of dementia in the community (4-6). Pure vascular dementia, although uncommon, may result from cerebral infarcts (7).
However, in Alzheimer's disease (AD) patients, the contribution of vascular lesions to cognitive impairment is uncertain. Detection of vascular cognitive burden in AD may be helpful in differentiating between mixed dementia (AD with infarcts) and pure AD, and to allow strategies to prevent recurrent vascular injury.
The results from previous studies are inconsistent. Some studies have suggested that patients with AD and concomitant cerebrovascular lesions had poorer cognitive performance than those without (8-10), whereas other studies have suggested that vascular lesions did not have an important effect on the clinical features including cognitive performance (11-13). These differing findings may be the result of different examined stages of AD (10), relative small numbers (< 30) of AD patients with cerebral infarcts (8, 10-13), and exclusion of large infarcts (8, 12, 13).
Patients with cerebral infarcts are a heterogeneous group with respect to clinical evidence (symptomatic or silent), location, volume, and multiplicity. Therefore, a larger sample may be needed to study the influence on cognition (14). Additionally, the importance of clinical history of stroke, which is often neglected in autopsy-based AD studies, might be studied together with other radiological features of cerebral infarcts and other covariates of AD to elucidate the influence of cerebral infarct in AD (11-13). Separation of symptomatic infarcts from silent infarcts is important because they have a different clinical significance in daily practice. Here we have examined the relationship of symptomatic cerebral infarcts to cognition in AD using a large database including 16 yr of data from an Alzheimer's Disease Research Center (ADRC).
MATERIALS AND METHODS
Patient selection
The study population consisted of subjects enrolled in the ADRC at Columbia University Subjects underwent standardized clinical evaluation, which included a structured neurological and psychiatric examination, neuropsychological testing, laboratory tests, and neuroimaging. Diagnoses are determined at a weekly consensus conference. Diagnosis of AD is based on National Institute of Neurological Communicative Disorders and Stroke-Alzheimer's Disease and Related Disorders Association (NINCDS-ADRDA) criteria (15). Details about the process have been published elsewhere (16, 17).
Information on stroke history was obtained from the patient and/or caregiver through structured questions. Neurological findings supporting a history of a stroke were documented after examination. Clinical stroke was defined by either symptoms (history) or signs (examination) that were indicative of stroke. In recent years, nearly all subjects have undergone computed tomography (CT) or MRI as part of their clinical evaluation. The interpretation of the neuroimaging data by the neuroradiologist was blinded to patient information other than "dementia" and was encoded in a database. A radiological infarct was defined as an area of hypodensity on brain CT scan or hyperintensity on T2-weighted brain MRI scan accompanied by hypointensity on T1-weighted images (4). White matter T2 hyperintensities without T1 changes, or dilated perivascular spaces, were not considered to be cerebral infarcts. Symptomatic infarcts were defined as having both radiological infarcts and clinical history of stroke. Silent infarcts were diagnosed in those patients showing radiological infarct without clinical history of stroke.
Between July 1991 and November 2005, 1,781 patients were diagnosed with AD, and of these, 780 patients were excluded due to absence of information about stroke history (n = 86) and/or absence of information about brain imaging (n = 728). Among the remaining 1,001 AD patients, a clinical history of stroke was present in 107 patients, and radiological infarcts in 308 patients. Sixty-eight patients with both were considered as having symptomatic infarcts.
AD patients that were included in this study were less educated (11.1 vs 11.6 yr, P = 0.02), more likely to be Hispanic (27% vs 17%, P < 0.001), more likely to have hypertension (49% vs 41%, P = 0.003), and less likely to have heart disease (11% vs 14%, P = 0.02) than the 780 excluded AD patients. There were no significant differences between the included and excluded AD patients regarding age, gender, and the proportion with diabetes mellitus.
Neuropsychological evaluation
In order to evaluate the influence of symptomatic cerebral infarcts on the cognitive performance of AD patients, selected neuropsychological tests were grouped into the following cognitive domains and converted into domain measures (16, 17). The memory domain included the total recall and delayed recall of the Selective Reminding Test and the recognition components of a multiple-choice version of the Benton Visual Retention Test. The executive function domain included phonemic fluency (a controlled oral word association test) and categorical fluency (animals and vegetables). The language domain included the total naming score for 15 selected items from the Boston Naming Test and the first 6 items from the repetition and comprehension subsets of the Boston Diagnostic Aphasia Examination. The visuospatial domain included the 5-item Rosen Drawing Test and the matching component of the multiple choice version of the Benton Visual Retention Test. The abstract reasoning domain included the age-scaled score of the revised Wechsler Adult Intelligence Scale (WAIS-R) similarities subtest and the identities and oddities subtest of the Dementia Rating Scale.
In order to define the cognitive domains, the results of each of the 12 baseline individual tests were first transformed into z-scores. Mean and standard deviations (SDs) for each test were calculated from the scores of 500 age-gender-matched subjects from the same ADRC data set who had neither dementia nor amnestic mild cognitive impairment nor non-amnestic mild cognitive impairment according to consensus at the consensus conference. There were no significant differences between AD patients and controls regarding age, gender, duration of education, ethnicity, and frequency of silent or symptomatic infarcts. Mean z-scores for each cognitive domain were calculated. Some individual test scores were missing; however, the domain measure was calculated when at least half of the individual scores were available.
Statistical analyses
We compared the demographic features of AD patients according to the presence of symptomatic cerebral infarcts using a non-parametric test for continuous variables and chi-square test for categorical variables. We evaluated the influence of symptomatic infarcts on the scores of the each cognitive domain measures using linear regression. The first linear regression analyses included symptomatic infarcts as an independent variable and cognitive domain measures as dependent variables. These were adjusted for age, sex, education, and ethnicity. After initial analysis, additional covariates were added to the model. We adjusted for diabetes mellitus, hypertension, heart disease, and the clinical dementia rating. In further regression analyses, we additionally adjusted for silent infarct, multiplicity of radiological infarcts, and location of radiological infarcts.
Ethics statement
This study was approved by the institutional review board of the New York State Psychiatric Institute (Protocol #5467R). All subjects gave informed consent for participation in this study. This study followed Good Clinical Practice, consistent with the International Conference on Harmonization (ICH) ethical principles for medical research involving human subjects, and with full compliance with privacy principles.
RESULTS
Sample characteristics
By NINCDS-ADRDA criteria, there were 522 probable AD patients and 479 possible AD patients. Most of the latter were designated as possible due to the presence of concomitant vascular or psychiatric dysfunction. Severity of dementia, classified by Clinical Dementia Rating (CDR) scale, was CDR 1 in 726 patients (72.5%), CDR 2 in 206 patients (20.6%), and CDR 3 in 69 patients (6.9%). A total of 503 infarcts were detected in the following locations: frontal 34; temporal 14; parietal 28; occipital 17; thalamus 51; basal ganglia 106; white matter 161; brainstem 27; cerebellum 32, and unclassified 33. Among 308 patients with radiological infarcts, 188 patients had a single lesion and the remaining 120 patients had multiple lesions. Neuroimaging, included MRI was performed in 59.9% of patients and CT alone in 40.1% of patients. The time between brain imaging and neuropsychological evaluation was somewhat greater for CT (9.9 ± 18.9 months) compared to MRI (7.2 ± 13.7 months, P = 0.01).
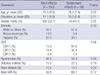
AD patients with symptomatic infarcts were older than those without (P = 0.03). Comparisons of other characteristics were not different between groups including imaging modality usage and duration between neuropsychological evaluation and neuroimaging (Table 1).
Influence of symptomatic infarcts on cognitive performance in AD
AD patients with a symptomatic infarct had poorer scores for executive function, irrespective of adjustment for age, gender, education, and ethnicity. This significance was persistent after four additional adjustments with vascular risk factors (hypertension, diabetes, and heart diseases) and CDR, silent infarct, multiple infarct, and frontal infarcts (Table 2). AD patients with a symptomatic infarct also had poorer scores in language and visuospatial performance after adjustment for age, gender, education, ethnicity, and multiple infarcts, but not in the other analyses.
Silent infarcts, multiple infarcts, and frontal infarcts had no discernible influence on any cognitive performance. Other locations of infarcts could not be added to the model due to inadequate of model fitness (variance inflation > 10).
When the analysis was limited to 962 patients by excluding those who had history of stroke without radiological infarcts, AD patients with a symptomatic infarct still had poorer scores for executive function in all models. When the analysis included only the 553 patients who had undergone MRI within one year of testing, AD patients with symptomatic infarcts still had poorer scores for executive function (β, -0.15; 95% CI: -0.60 to -0.09; P = 0.01). Only 4 patients had symptomatic infarcts among the 522 patents with probable AD and the influence of symptomatic infarcts disappeared in the separated analysis in probable AD patients.
DISCUSSION
Consistent with results from other studies of non-demented elderly (4-6, 18), symptomatic infarcts in patients with AD likewise had an additional unfavorable influence on cognition, even after considering the severity of AD. This result is consistent with described cognitive changes after symptomatic stroke in AD (19, 20). A decline in executive performance was noted regardless of the multiplicity or location of infarcts, within the limits of this study. Executive dysfunction may be related to injury to the frontal-subcortical network, or possibly related to other infarct locations (21).
We did not find a detrimental effect of silent radiological infarcts in AD patients, unlike some studies of non-demented elderly or patients with mild AD (4, 10). Usually, silent infarcts have a smaller volume and are located in non-eloquent areas compared to symptomatic infarcts; therefore, it is difficult to detect minimal changes resulting from minor infarcts, especially in severe or neocortical stage AD.
The strengths of our study included a large multiethnic referral population, separate consideration of symptomatic infarcts and silent infarcts, examination of several cognitive domains, and adjustment for multiple covariates. There are also a number of limitations to this study. First, we were unable to examine the various factors that may have influenced the associations identified, such as the timing of symptomatic infarcts, subtypes of stroke, the presence of white matter hyperintensities (22). Second, numbers of patients with severe dementia are small compared to those with mild to moderate dementia. Also, there are many fewer patients with symptomatic cerebral infarcts, than with silent infarcts, althouth this reflects actual prevalences (11). Third, we do not have validation of diagnosis of AD with autopsy findings, so there is a possibility of misdiagnosis of vascular dementia as AD. However, AD patients with symptomatic infarcts apt to be classified into possible AD regardless of burden of AD pathology. Therefore, it might be impossible to study the influence of symptomatic infarct after excluding possible AD patients. Finally, the analysis here involves data accumulated over a 16 yr (1991-2005), with accompanying difference in imaging modalities and varying time intervals between neuroimaging study and the neuropsychological evaluation. Additionally, executive function was not evaluated by the other tests for frontal-executive function (23).
Despite these potential limitations, our results support the hypothesis that symptomatic cerebral infarcts in the AD population may provide an additive "non-memory" factor contributing to dementia and the influence of cerebral infarcts is neither general nor diffuse, and the presence of clinical history may have a more important influence on executive performance in AD.

 XML Download
XML Download