

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is usually progressive and is associated with an abnormal inflammatory response of the lung to noxious particles or gases (1). Previous studies have shown that regular treatment of COPD with an inhaled corticosteroid (ICS) improve pulmonary function and reduces the frequency of exacerbations, even though it does not modify the long-term decline of forced expiratory volume in 1 sec (FEV1) (2, 3). Combination therapy with an ICS and a long acting β2-agonist (LABA) is better in improving lung function and health status, and reducing daily symptoms and exacerbations than single therapy (4, 5).
COPD is a heterogeneous disease in terms of clinical, physiological, and pathological presentation. The chronic airflow limitation associated with COPD is caused by a variable contribution of small airway disease (obstructive bronchiolitis) and parenchymal destruction (emphysema). Thus, the therapeutic response to combination treatment with an ICS and a LABA is also variable. Previous COPD guidelines recommended the use of short-term (two weeks) oral corticosteroid therapy to identify COPD patients who might benefit from long-term treatment with an ICS (6). However, it was recently shown that the response to a short-term oral corticosteroid is a poor predictor of the longterm response to an ICS (7). Currently, there are no known good predictors of the responsiveness of COPD patients to treatment with an ICS and a LABA.
The aim of this study was to identify predictors of pulmonary function response to 3 months of treatment with salmeterol/fluticasone in patients with COPD.
MATERIALS AND METHODS
Patients
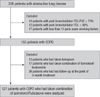
A total of 127 stable COPD patients who had been treated with salmeterol/fluticasone for 3 months were analyzed retrospectively. All patients were selected from the Korean Obstructive Lung Disease (KOLD) Cohort, which had 226 stable patients with obstructive lung disease (OLD) were prospectively recruited from the pulmonary clinics of 11 hospitals in Korea from June 2005 to September 2009 (Fig. 1). The inclusion criteria for the KOLD cohort have been described elsewhere (8). COPD was diagnosed based on smoking history (more than 10 pack-years) and the presence of airflow limitation that was not fully reversible (post-bronchodilator FEV1/forced vital capacity [FVC] < 70% and post-bronchodilator FEV1 < 80% predicted). We included COPD patients who had wheezing history or who showed partial reversibility of airflow limitation after inhalation of salbutamol.
Study protocol
Baseline clinical data were obtained after cessation of the following respiratory medications: an ICS for 2 weeks, an inhaled LABA for 2 days, an inhaled short-acting β2-agonist or inhaled short-acting anti-cholinergic for 12 hr. The baseline clinical data included demographic data, smoking history, chronic bronchitis history, wheezing history, pulmonary function tests, chest radiography and volumetric computed tomography (CT). Chronic bronchitis was defined as cough and sputum production on most days for a minimum of 3 months per year for at least 2 yr (9). Wheezing history was obtained through the following question: "Have you had wheezing or whistling in your chest at any time in the last year?" (10) Atopic status was assessed by a skin prick test to 11 common allergens, with a 10% histamine and saline control. Patients were considered to be atopic if they reacted with a wheal of larger than the histamine control for more than one of the allergens. After obtaining baseline data, patients were treated with a salmeterol/fluticasone propionate 50/500 µg dry powder inhaler twice per day for 3 months, and then spirometry and lung volume measurement were performed again after the morning medication. During the 3-month treatment period, only salbutamol was allowed as needed. Adherence to the treatment medication monitored and recorded by research coordinators.
Pulmonary function tests
Spirometry was performed using a Vmax 22 instrument (Sensor-Medics; Yorba Linda, CA, USA) or a PFDX machine (MedGraphics, St. Paul, MN, USA). To assess the post-bronchodilator change, spirometry was performed pre-bronchodilator and 15 min after inhalation of salbutamol (400 µg) through a metered-dose inhaler (MDI) with a spacer. Lung volumes were measured by body plethysmography (V6200; SensorMedics, or PFDX). Diffusing capacity for carbon monoxide (DLco) was measured by the single-breath method using a Vmax229D (Sensor-Medics) or a Masterlab Body (Jaeger AB, Würtsburg, Germany). The predicted values of FEV1, forced vital capacity (FVC), FEV1/FVC and DLco were calculated from Korean equations formulated using data from a healthy non-smoking population (11, 12). The predicted values of lung volumes were calculated from ECSC equations (13). All pulmonary function tests were performed as recommended by the American Thoracic Society/European Respiratory Society (ATS/ERS).
Computed tomography
Volumetric CT scans were performed using 16-slice multi-detector CT (MDCT) scanners, according to previous described scanning protocols (14). Image data were stored in the Digital Imaging and Communications in Medicine (DICOM) format. Using in-house software, images of the whole lung were extracted automatically and the attenuation coefficient of each pixel was measured and calculated. The cutoff level between normal lung density and a low-attenuation area (LAA) was defined as -950 HU (15). From the CT data, the volume fraction of the lung below -950 HU (V950) was calculated automatically. The airway dimensions, wall area (WA), lumen area (LA) and wall area percent (WA%, defined as WA/[WA + LA] × 100), were measured near the origin of two segmental bronchi (right apical and left apico-posterior) selected by a consensus reading of two radiologists. The software automatically detects the airway lumen and the inner and outer boundaries of the airway wall by use of a full-width-half-maximum (FWHM) method (16). The mean value of each segmental bronchus was used for analysis.
Statistical analysis
To investigate factors associated with the initial maximal positive pulmonary function response to 3 months of treatment with salmeterol/fluticasone, changes in pre-bronchodilator FEV1, FVC and inspiratory capacity (IC)/total lung capacity (TLC) before and after 3 months were used as the dependent variable in univariate and multivariate analyses. The FEV1 and FVC changes were expressed as % of predicted normal values (% predicted) to avoid the potential problem that baseline FEV1 and FVC appear to influence on FEV1 and FVC changes if expressed as % of baseline (17). Selected independent variables were sex, age, body mass index (BMI), chronic bronchitis history, wheezing history, smoking status (current or ex-smokers, smoking pack-years), pulmonary function parameters and CT parameters. For data had a normal distribution, we used Student's t-test or a oneway analysis of variance (ANOVA) for categorical variables. For data that had a non-normal distribution, we used Mann-Whitney U test or the Kruskall-Wallis test for categorical variables. Relationships between two continuous variables were examined by Pearson's correlation analysis. The prediction models for pulmonary function response to 3 months of treatment with salmeterol/fluticasone were constructed from multiple, stepwise, linear regression models. All statistical analyses were performed with the SPSS statistical package (version 12.0, SPSS Inc, Chicago, IL, USA), and P values less than 0.05 were considered significant.
RESULTS
Patient characteristics
Table 1 lists the baseline characteristics of the 127 COPD patients. Of the enrolled patients, 123 (97%) were male. Mean age was 65.5 (SD: 7.6) yr, and mean smoking history was 46.3 (20.7) pack years. A total of 74 patients were classified as GOLD II (moderate COPD), 46 as GOLD III (severe COPD), and 7 as GOLD IV (very severe COPD). Ninety-one percent of subjects indicated that they had taken over 80% of the recommended medication dose.
Univariate analysis of baseline clinical variables and pulmonary function response to 3 months of treatment with salmeterol/fluticasone
The FEV1, FVC and IC/TLC changes after 3 months of treatment were normally distributed without evidence of a separate responder group. The mean FEV1, FVC and IC/TLC changes after 3 months of the treatment were 0.160 (0.223) L, 5.1 (7.3)% predicted and 0.202 (0.380) L, 4.8 (9.0)% predicted, and 2.7 (6.1)%, respectively. There were no significant differences in the mean postbronchodilator FEV1 and FVC changes according to baseline GOLD severity stage. Patients with GOLD stage III or IV showed significantly larger TLC and functional residual capacity (FRC) reduction after the 3 months of treatment with salmeterol/fluticasone than patients with GOLD stage II. However, there were no significant differences in the mean FEV1, FVC and IC/TLC changes after 3 months of the treatment (Table 2).
Among categorical variables, COPD patients with wheezing history had significantly greater FEV1 and FVC changes after 3 months of treatment than those without wheezing history (7.8% vs 2.7% predicted for FEV1, P < 0.001; 7.3% vs 2.3% predicted for FVC, P = 0.002). Simple correlation analysis indicated that pre-bronchodilator FEV1 and FVC had a weak negative correlation with the FEV1 and FVC changes after 3 months of the treatment but that post-bronchodilator FEV1 and FVC had no significant correlation with FEV1 and FVC changes after 3 months of the treatment. The post-bronchodilator FEV1 and FVC changes had a positive correlation with the FEV1 and FVC changes after 3 months of the treatment. LAA had a weak negative correlation with the FEV1 change after 3 months of the treatment, but mean WA was not correlated with the FEV1, FVC and IC/TLC changes after 3 months of the treatment (Table 3).
Prediction models for pulmonary function response to 3 months of treatment with salmeterol/fluticasone
Multiple, stepwise, linear regression analysis showed that four variables, wheezing history, pre-bronchodilator FEV1, post-bronchodilator FEV1 change, and LAA were independently associated with the FEV1 change after 3 months of the treatment (R = 0.578). Multiple, stepwise, linear regression analysis also showed that two variables, pre-bronchodilator FVC and post-bronchodilator FVC change were independently associated with FVC change after the 3-month treatment (R = 0.533), and pre-bronchodilator IC/TLC and post-bronchodilator FEV1 change were independently associated with IC/TLC change after 3 months of the treatment (R = 0.401, Table 4).
DISCUSSION
Our results show that wheezing history, baseline pulmonary function, bronchodilator responsiveness, and emphysema extent on CT could be used for predicting the pulmonary function response to 3 months of treatment with salmeterol/fluticasone in patients with COPD. This allowed us to make a significant prediction model for FEV1, FVC and IC/TLC changes after 3 months of treatment.
The response of pulmonary function to an ICS and a LABA in COPD patients has been well established in previous studies (4, 5). Current guidelines recommend combination of an ICS and a LABA for symptomatic COPD patients with post-bronchodilator FEV1 < 50% predicted and repeated exacerbation (1). However, clinical benefits from combination pharmacotherapy are not restricted to patients of severe stage of disease (18, 19). It has been difficult to predict which patients will show better responses to an ICS and a LABA. In this study, COPD patients with wheezing history, lower baseline lung function, larger bronchodilator responsiveness and lower LAA on CT responded better to the treatment with salmeterol and fluticasone. This combination would be expected to be more effective in improving the small airway component (chronic obstructive bronchiolitis) of COPD.
Wheezing is the most common symptom reported by asthmatic patients, but is also commonly reported by COPD patients (20). Marini et al. (21) reported that wheezing patients with chronic airflow obstruction differed from non-wheezing patients with chronic airflow obstruction by their bronchodilator response. Our results showed the COPD patients with a wheezing history had a significantly higher mean FEV1 and FVC changes after bronchodilator and 3 months of treatment than those without such a history. Our study also showed a positive correlation between bronchodilator responsiveness (post-bronchodilator FEV1 and FVC changes) and the FEV1 and FVC changes after 3 months of treatment. Previous studies showed that corticosteroid reversibility in COPD patients was related to features of asthma (22). Recently, Kitaguchi et al. (23) also reported that wheezing and bronchodilator responsiveness were significant determinant for the reversibility in response to an ICS.
This study also showed that COPD patients with lower pre-bronchodilator FEV1 and FVC have better responses to our combination treatment. On the contrary, there was no significant effect of post-bronchodilator FEV1 on the response to combination treatment. A post-hoc analysis in the TORCH study showed similar results in that the severity of COPD which was assessed by post-bronchodilator FEV1 was not related to the FEV1 improvements after a combination treatment (19). This result might be explained as follows. The lack of a relation between COPDseverity and treatment responsiveness may be caused by the fact that pre-bronchodilator FEV1 and post-bronchodilator FEV1 change relate to treatment responsiveness. The post-bronchodilator FEV1 and FVC (which is unrelated to responsiveness) are the sum of the value of pre-bronchodilator FEV1 and FVC (which is related to responsiveness) and the post-bronchodilator FEV1 and FVC changes (which is related to responsiveness).
CT provided an objective method for measuring the extent and severity of emphysema (15, 24). Several recent studies indicated that it is possible to separate COPD patients into emphysema-dominant and airway-dominant phenotypes by use of high resolution CT (HRCT) (23, 25, 26). Kitaguchi et al. (23) reported that lower total LAA score and the grade of bronchial wall thickening were significant determinants for bronchodilator responsiveness and for the responsiveness to the treatment with an ICS. However, other two studies found no significant differences in bronchodilator responsiveness among groups classified according to severity of emphysema (25, 26). Previously, our study group has shown that emphysema dominant COPD patients (LAA ≥ 20% and pre-bronchodilator FEV1 ≥ 45% predicted) responded poorly to the 3 months of combination treatment (27). In this study, LAA had a week negative correlation with the FEV1 change after 3 months of the treatment. This result might be explained as follows. For COPD patients, the major determinants of FEV1 are small airway disease and emphysema. If a COPD patient has a more significant emphysema component than that of small airway disease, he or she would be expected to have a poorer response to pharmacologic treatments that predominantly target small airway disease. In this study, mean WA was not correlated with the FEV1 and FVC change after 3 months of the treatment. A previous report showed that large airway dimension serve as a useful surrogate for small airway remodeling (28). Nonetheless, it is possible that the lack of a significant relationship between WA and treatment response may be due to the relatively imprecise and indirect estimate of small airway wall area. There are two factors that could have potentially confounded our volumetric CT result. First, we used three different MDCT scanners, and different scanners may have graded the emphysema index differently. A method that corrects for differences between different CT scanners has not yet been established. Second, we used only two large airways to evaluate airway dimension.
In this study, 19.7% of included patients had overlapping diagnoses of COPD and asthma (overlap syndrome). Those patients with overlap syndrome could affect our study results. However, subgroup analysis after excluding patients with overlap syndrome showed the similar results. Our study has two limitations. First, we did not consider airway inflammatory markers. Previous studies showed an increased number of eosinophils in bronchoalveolar lavage fluid in a subset of patients with COPD who responded to short-term administration of oral corticosteroids (29) and sputum eosinophil counts were significantly correlated with reversibility in response to ICS treatment (23). If we had included airway inflammatory markers, we might have been able to develop more powerful prediction models. Second, 97% of our patients were male. Gender may have a substantial influence on treatment response in COPD patients (30), so we cannot generalize our results to females.
In conclusion, wheezing history, baseline pulmonary function, bronchodilator responsiveness, and emphysema extent in COPD patients may be used for predicting the pulmonary function response to 3 months of treatment with salmeterol/fluticasone.




 XML Download
XML Download