

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The presence of diabetes is an independent risk factor for atherosclerosis. Endothelial dysfunction, oxidative stress, and low-grade inflammation are major features in the pathophysiology of this disease (1). It has been shown that atherosclerosis in patients with diabetes mellitus (DM) can lead to acute coronary artery disease, ischemic cerebral disease, and peripheral arterial disease (2). Because atherosclerosis is an inflammatory process, several plasma markers of inflammation have been evaluated as potential tools for the prediction of risk for cardiovascular disease (3). For example, a high serum level of high-sensitivity C-reactive protein (hs-CRP), a marker of systemic inflammation and a mediator of atherosclerotic disease, has been correlated with an increased risk for cardiovascular disease (4-6).
Although it is generally accepted that hs-CRP levels can act as a predictor for cardiovascular disease in non-diabetic patients, there is a relative lack of data concerning the usefulness of hs-CRP levels when predicting the occurrence of cardiovascular diseases in Asian type 2 diabetic patients. Thus, the objective of this study was to clarify the independent clinical value of hs-CRP levels in the occurrence of major adverse cardiovascular event (MACE) in Korean type 2 diabetic patients.
MATERIALS AND METHODS
Participants and study design
A retrospective cohort study was conducted involving 2,452 patients between 30-70 yr of age with type 2 diabetes who were managed in the Endocrinology Department of Kwandong University Myongji Hospital, Goyang, Korea. Serum hs-CRP levels were measured between January 2004 and December 2007 during hospital visits prior to the occurrence of MACE. After careful history taking and physical examination, 388 subjects were excluded for the following reasons: previous cardiovascular diseases, type 1 diabetes, pregnancy, breast feeding, acute infection or chronic inflammatory disease (upper or lower respiratory infection, urinary tract infection, acute gastrointestinal infection, inflammatory bowel disease, osteoarthritis, rheumatoid arthritis, chronic hepatitis, gout, and bronchial asthma), or high baseline hs-CRP levels (> 1 mg/dL) (7). MACE occurrence was identified using an electronic medical record system in the remaining 2,064 subjects. All subjects were contacted by phone to confirm the occurrence of MACE. If the patients were confirmed with MACE but had moved to another hospital, the relevant hospital was contacted so that data could be collected. The occurrence and non-occurrence of MACE were confirmed in 1,766 of the 2,064 subjects. The mean follow-up period was 55.5 (20-92) months.
Baseline measurements and definitions
Blood sampling and hemodynamic measurements were performed on all patients. Levels of hs-CRP were measured using a high-sensitivity assay (turbidity immune assay, Toshiba, Tokyo) with a detection limit of 0.01 mg/dL. DM was defined as a fasting blood glucose concentration of ≥ 126 mg/dL or as receiving anti-hyperglycemic drug treatment. Body mass index (BMI) was calculated by weight in kilograms divided by square of height in meters. Height, weight, and plasma levels of hs-CRP, fasting glucose, HbA1c, total cholesterol, triglycerides, and high-density lipoprotein (HDL)-cholesterol were measured simultaneously. LDL-C was estimated using the equation developed by Friedewald et al. (8) Regular physical activity was defined as over 150 min of exercise per week.
Myocardial infarction (MI) was defined according to the guidelines of the American Heart Association/American College of Cardiology and included elevated cardiac enzymes and specific electrocardiogram changes (9). Percutaneous coronary intervention (PCI) was defined as needing percutaneous transluminal coronary angioplasty or stent insertion against significant stenosis of the coronary artery. A stroke was defined as rapidly-developing loss of brain function due to disturbance in blood supply to the brain. Additionally, according to the standard World Health Organization definition, a stroke is limited to a focal neurological deficit over 24 hr and cerebral hemorrhage on brain imaging was excluded (10). Peripheral vascular angioplasty, peripheral vascular surgery, and amputation due to critical limb ischemia were considered to be peripheral vascular events. Cardiovascular death was limited to the diagnostic code I21-25 or I60-73 for the cause of death. Thus, MACE included cases of MI, coronary obstructive disease treated by PCI or CABG, stroke, other vascular diseases treated by angioplasty or vascular surgery, and cardiovascular death.
Statistical analyses
Several variables, including hs-CRP levels, fasting glucose, HbA1c, total cholesterol, triglycerides, HDL-cholesterol, and LDL-cholesterol were not normally distributed in the Shapiro-Wilk test. Logarithmic transformation was used to normalize them and the variables were applied to the following analysis. A logistic regression analysis and a general linear model were used to compare trisected hs-CRP levels and clinical characteristics after adjusting for age, sex, and duration of diabetes. The patients were divided into two groups according to whether MACE occurred or not and the clinical characteristics between the two groups were compared through a general linear model and a logistic regression analysis after adjusting for age, sex, and duration of diabetes. The hazard ratios were estimated for MACE according to the tertile of baseline hs-CRP levels after adjusting for age, sex, duration of diabetes, current smoking, physical activity, and total cholesterol by Cox regression analysis.
RESULTS
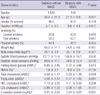
The clinical characteristics of the patients are shown in Table 1. The mean hs-CRP level for the 1,766 subjects was 0.21 ± 0.22 mg/dL and the median value was 0.13 mg/dL (interquartile range 0.05-0.28). Enrolled subjects were divided into three groups according to serum hs-CRP level (mg/dL); low (< 0.08 mg/dL), medium (0.08-0.21 mg/dL), and high (> 0.21 mg/dL). The low, medium, and high hs-CRP levels were 46.2%, 45.8%, and 48.6% in women and there was no significant difference of sexual distribution between the groups. The duration of DM and LDL-cholesterol level were not different between the groups. The result showed no significant difference in frequency of angiotensin converting enzyme-inhibitors, angiotensin receptor blocker, statin, aspirin and clopidogrel administration. However, age, weight, BMI, blood pressure, fasting blood glucose, HbA1c, total cholesterol, and triglycerides increased in proportion to the level of hs-CRP. HDL-cholesterol showed an inverse proportion to the level of hs-CRP. The percentage of regular physical activity was low in the high hs-CRP group compared with the other groups.
MACE was observed in 144 patients during the follow-up period (mean of 55.5 months). MI was seen in 19 patients; 106 patients were treated by PCI due to coronary arterial obstructive disease, and stroke occurred in 25 patients. All-cause death occurred in 50 patients; 15 of cardiovascular disease, 10 of malignancy, 13 of infectious diseases, 10 of other diseases, and two of unknown causes.
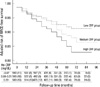
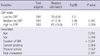
Subjects were divided into two groups according to whether MACE occurred or not. Age, duration of DM, current smoking, physical activity, total cholesterol, and hs-CRP levels were greater in subjects with MACE. There were no significant differences in gender, past smoking, BMI, blood pressure, fasting blood glucose, HbA1c, triglycerides, HDL-cholesterol, or LDL-cholesterol (Table 2). Compared with the low-level hs-CRP group, the medium- and high-level hs-CRP groups exhibited a trend towards an increased risk for MACE in a Cox model (Fig. 1). The crude hazard ratio was 1.44 (0.92-2.24) for the medium level hs-CRP group and 2.00 (1.31-3.04) for the high level hs-CRP group. After adjusting for age, sex, duration of DM, current smoking, physical activity, and total cholesterol, the relative risk of MACE increased by 77% in the high-level hs-CRP group compared with the low-level hs-CRP group (1.16-2.71). The hazard ratio of MACE for the medium-level hs-CRP group compared with the low-level hs-CRP group was not significant (Table 3).
DISCUSSION
The aim of this study was to examine the relationship between hs-CRP levels and the prognosis of MACE in patients with type 2 diabetes and without cardiovascular disease. The predictive value of baseline hs-CRP levels in the prognosis of MACE was lower than that of age or duration of DM, but higher than physical activity, current smoking, and other conventional risk factors for cardiovascular disease.
Many prospective studies have shown that a high serum concentration of LDL-cholesterol is a major risk factor for coronary heart disease (11). However, patients with type 2 diabetes show a characteristic lipid profile of normal or only slightly raised LDL-cholesterol (12). Increased small, dense LDL particles may perform a more important role during the occurrence of macrovascular complications than the total concentration of LDL-cholesterol in type 2 diabetic patients (13). Indeed, in some cohorts of DM patients, total cholesterol and LDL-cholesterol levels were not associated with cardiovascular risk, whereas high triglyceride levels and low HDL-cholesterol concentrations were powerful predictors of coronary heart disease (14). The effect of hypertension in deaths from coronary heart disease is increased by 2-5-fold in diabetic patients and the United Kingdom Prospective Diabetes Study confirmed the beneficial effects of improved blood pressure control in type 2 diabetic patients (15). However, the present findings showed no difference in baseline lipid profiles or blood pressure in patients with or without MACE. Currently, the widespread use of lipid-lowering and anti-hypertensive agents in patients with type 2 diabetes may lower the value of baseline lipid profiles and blood pressure in the prediction of the risk for cardiovascular disease. Nevertheless, hs-CRP levels were more associated with MACE than lipid profiles or blood pressure. It is suggested that hs-CRP levels are less affected by other confounding factors, such as medication, when determining risk of future cardiovascular events in type 2 diabetic patients.
It has been reported that hs-CRP levels are higher in patients with type 2 diabetes than in patients without DM (16). However, there were differences in the serum hs-CRP levels of subjects without diabetes based on ethnicity (17-19). In patients with type 2 diabetes this same tendency may exist. Mean values of hs-CRP levels in type 2 diabetic subjects have been reported to be 0.68 mg/dL in American Caucasians, 0.11 mg/dL in Japanese, and 0.19 mg/dL in Chinese populations (16, 20, 21). Median hs-CRP levels of Italian patients with type 2 diabetes were reported as 0.26 mg/dL (22). In the current study, mean and median hs-CRP levels in Korean patients with type 2 diabetes were 0.21 mg/dL and 0.13 mg/dL, respectively, suggesting that hs-CRP levels in European and American Caucasians may be 2-4 times higher than in Asian patients. Body weight may be an important factor in this difference. The average level of hs-CRP is quite different according to BMI and gender of the subjects (23). In fact, body weight influenced levels of hs-CRP in the current study and BMI ranges of Asian, European, and American patients with type 2 diabetes mellitus were 24 to 26, 26 to 31, and 31 to 35 in the above-mentioned reports. Thus, it is important that a clinician consider weight and ethnicity when using hs-CRP levels as a marker of cardiovascular risk.
In non-diabetic Caucasians, it is known that hs-CRP levels of > 0.3 mg/dL may have predictive qualities (24). In European and American type 2 diabetic patients, those with a level of 0.3 mg/dL or greater had significantly higher relative risks for cardiovascular events, coronary heart disease, and cardiovascular mortality (22, 25, 26). In the present study, the hazard ratio for MACE was 1.47 (95% CI; 1.02-2.10) when considering the hs-CRP cutoff point of > 0.3 mg/dL. However, this cutoff point for cardiovascular disease events is not appropriate for Asian patients with type 2 diabetes because only 22.3% of these patients exhibited an hs-CRP level of > 0.3 mg/dL and 69.7% of MACE occurred in the low risk group in this study (data not shown). To date, few studies have reported findings concerning hs-CRP levels and related cardiovascular events in Asian type 2 diabetic patients. In Japanese patients with type 2 diabetes, the highest tertile of hs-CRP levels (> 0.11 mg/dL) had a relative risk of 1.31 (95% CI: 1.04-1.67) for all-cause death and cardiovascular events (21). Here, the cutoff point for the highest hs-CRP tertile was 0.21 mg/dL and higher than that of Japanese patients with type 2 diabetes. The difference in BMI between these studies may play a role in the findings (25.1 vs 23.7) but ethnic difference must also be considered.
It has been reported that the more risk factors for metabolic syndrome are clustered, the greater the severity of coronary artery disease will be (27). This may be applied to the extended disease concept of MACE. Thus, a global risk assessment for cardiovascular disease has meaningful implications for preventing future occurrences of MACE. Hs-CRP measurements might provide information for a global risk assessment for cardiovascular disease. Patients with high hs-CRP levels should be made aware of an increased risk for MACE and be more closely monitored and treated. For patients with coronary artery disease, the reduced rate of progression of atherosclerosis associated with intensive statin treatment, compared with moderate statin treatment, is related to greater reductions in the levels of both atherogenic lipoproteins and hs-CRP (28, 29). Moreover, in Korea, the early prescription of statins has been reported to improve prognosis in acute ischemic stroke cases (30).
Although this study used a large cohort of patients with type 2 diabetes, there are some limitations. This is a retrospective cohort study; thus, some events might be omitted because of errors in medical records or patient memories. Secondly, only baseline data were analyzed in this study and it was not reflected in the outcome any change in cardiovascular risk factors and the administration of statin, aspirin, anti-platelet agent during the follow-up period. Additionally, the fact that baseline hs-CRP was not followed up could be also a limitation to analyze the outcome.
In conclusion, the high-level hs-CRP tertile of > 0.21 mg/dL is independently associated with the future incidence of MACE in Korean patients with type 2 diabetes and without present cardiovascular disease. But, it did not suggest hazard ratio was proportional to hs-CRP level because the hazard ratio of MACE in subjects whose hs-CRP levels were > 0.3 mg/dL was lower than one in subjects whose hs-CRP levels were > 0.21 mg/dL.

 XML Download
XML Download