

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Although drug-eluting stent (DES) use has remarkably reduced in-stent restenosis (ISR) and neointimal hyperplasia, percutaneous coronary intervention (PCI) of diffuse long coronary artery lesions remains challenging (1, 2); these lesions are commonly encountered in routine clinical practice and often lead to use long stented segments with stent overlap. Because stented segment length was a known independent predictor of ISR in the bare-metal stent (BMS) era and limited data are available on the long-term efficacy and safety of DES in diffuse long coronary artery lesions, we investigated the long-term efficacy and safety of DES in diffuse long lesions (3-5).
MATERIALS AND METHODS
Study population
From May 2006 to May 2007, a total of 335 consecutive patients (374 lesions) underwent PCI with implantation of long DES (≥ 30 mm) in de novo long coronary artery lesions at 3 cardiac centers (Inje University Busan Paik Hospital in Busan, Yeungnam University Medical Center in Daegu and Keimyung University Dongsan Hospital in Daegu) in Korea. Patients were divided into sirolimus-eluting stent (SES, Cypher, Cordis, Johnson & Johnson, Roden, The Netherlands, n = 218) and paclitaxel-eluting stent (PES, Taxus, Boston Scientific Corp, Natick, MA, USA, n = 117) recipient groups, and 8-month angiographic 2-yr clinical outcomes were compared.
Procedures and medications
All interventions were performed using standard techniques. DES selection, Glycoprotein IIb/IIIa inhibitors and intravascular ultrasound (IVUS) were used at the discretion of the operator. All patients received a loading dose of 300 mg clopidogrel followed by a daily dosage of 75 mg for 12 months, in addition to life-long aspirin therapy.
Follow-up
Angiographic follow-up was recommended for all living patients at 8 months after index procedure. Clinical follow-up was performed for all patients at 1, 3, 6, 9 and 12 months, and every 3 months thereafter either during out-patient department visits or by direct telephone calls to patients.
Study outcomes and definitions
Study outcome was a composite of major adverse cardiac events (MACE) including cardiac death, myocardial infarction (MI), target-lesion revascularization (TLR), target-vessel revascularization (TVR) and stent thrombosis (ST).
Procedural success was defined as residual diameter stenosis ≤ 30% and the absence of any-in hospital MACE. MI was diagnosed when cardiac enzyme (creatine kinase MB fraction) levels were elevated more than threefold the normal level, with chest pain lasting ≥ 30 min, or with the appearance of new electrocardiographic changes, or with imaging evidence of new regional wall motion abnormality or loss of viable myocardium. TLR was defined as either surgical or percutaneous reintervention driven by significant (> 50%) luminal diameter narrowing within the stent or the 5 mm borders proximal and distal to the stent and undertaken in the presence of either anginal symptoms or objective evidence of ischemia. TVR was defined as revascularization within the target vessel encompassing the target lesion. Stent thrombosis (ST) was classified by the Academic Research Consortium definition as definite, probable, or possible and as acute (0 to 24 hr), subacute (> 24 hr to 30 days), late (> 30 days to 1 yr) or very late (> 1 yr). ST was defined as 1) definite: an acute coronary syndrome with angiographic documentation of either vessel occlusion or thrombus within or adjacent to a previously successfully stented vessel or autopsy evidence of stent thrombosis, 2) probable: acute MI in the distribution of the treated vessel or unexplained death < 30 days after the index PCI and 3) possible: unexplained death > 30 days after the index PCI (6, 7).
Angiographic restenosis was defined as ≥ 50% of a diameter stenosis. Cumulative rates of event-free survival and MACE were analyzed over a two-year follow-up period.
Quantitative coronary angiographic analysis
The percentage of diameter stenosis, minimal lumen diameter, lesion length and reference diameter were analyzed with an automated edge-detection system (CASS II, Pie Medical, Maastricht, The Netherlands) before the procedure, after the procedure, and at follow-up. Lesion morphology was defined according to the guidelines of the American College of Cardiology and the American Heart Association (8).
Statistical analysis
Data are expressed as mean ± SD for continuous variables, and as frequencies for categorical variables. A two tailed Student's t test was used to assess differences between continuous variables. The chi-square (χ2) test was used for comparison of categorical variables. Multivariate logistic regression analysis was carried out using the baseline clinical and angiographic characteristics to identify the independent predictors of MACEs. The following variables were tested; pre-lesion length, overlapping, number of stents in long lesion, multi-vessel disease and used stent type. Major adverse cardiac event-free survival distributions were estimated according to the Kaplan-Meier method. The log-rank test was used to compare MACE-free survival between two groups. Probability values < 0.05 were considered significant. Data were analyzed with SAS 9.1.3. (SAS Institute Inc., Cary, NC, USA).
RESULTS
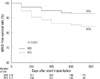
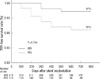
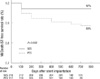
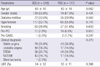
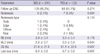
Baseline characteristics of the patients are presented in Table 1 and there were no significant differences between groups. Angiographic and procedural data are shown in Table 2; most lesions were type C according to the American College of Cardiology and American Heart Association and guidelines (8). Mean lesion length (40.4 ± 14.3 mm in SES and 43.6 ± 15.2 mm in PES, P = 0.063) and mean stent length (44.9 ± 15.2 mm in SES and 47.4 ± 15.9 mm in PES, P = 0.121) did not differ significantly between groups. Post-procedural diameter stenosis was greater in the PES than that in SES group (6.1% ± 4.2% in SES vs 7.9% ± 5.0% in PES, P = 0.001). Angiographic follow-up at 8 months was performed in 47.3% and binary restenosis rate was 2.1% in the SES and 5.3% in the PES group (P = 0.094). Late loss was significantly lower in the SES than in the PES (0.4 ± 0.6 mm in SES vs 0.7 ± 0.8 mm in PES, P = 0.007, Table 3). Mean clinical follow-up duration was 849 ± 256 days. In-hospital MACE rates were not statistically different between groups (1.8% in SES vs 2.6% in PES, P = 0.656, Table 4). During hospitalization, 4 patients in the SES group died; 2 with cardiogenic shock, 1 with cardiogenic shock and acute stent thrombosis, and one with cardiac tamponade, while two patients in the PES group died of cardiogenic shock after acute myocardial infarction (Table 4). At one-month follow-up, one additional patient died after subacute stent thrombosis in the SES group, and likewise in the PES group (Table 4). At one year follow-up, two additional deaths occurred in the PES group related to late stent thrombosis, while there were no deaths in the SES group. At two-year follow-up, two additional deaths were found in the PES group related to heart failure; however, there were no additional cases of stent thrombosis (Table 4). Cumulative total MACE showed SES yielded superior results than PES (5.5% in SES vs 15.4% in PES, P = 0.003). MACE-free survival rates are presented in Figs. 1, 2 shows TVR-free survival and Fig. 3 shows myocardial infarction, death and stent thrombosis free survival.
From test variables with pre-lesion length, overlapping, number of stents in long lesion, multi-vessel disease and used stent type, the independent risk factors of MACE for diffuse long coronary artery lesions were used stent (P = 0.003, odds ratio 3.181, C.I. 1.492-6.779) and overlapping stent (P = 0.025, odds ratio 1.790, C.I. 0.814-3.937).
DISCUSSION
The major finding of this study is that long-term follow-up of DES implantation in diffuse long coronary lesions showed acceptable low rates of clinical events, with SES being more effective and safer than PES in this real-world clinical experience.
Restenosis remains a major problem in treating with DES use, particularly in off-label usage such as in diffuse long lesions. Stent type can affect the risk of restenosis and SES is superior in terms of late loss and restenosis (9, 10).
Lee et al. (11) reported that the full metal jacket DES method was safe and effective in the treatment of diffuse long coronary artery disease with restenosis rates of 11.1% and 22.2% for SES and PES, respectively, suggesting that the risk of restenosis is influenced by the type of DES used. Kim et al. (12) also reported that for patients with long coronary artery disease, SES implantation was associated with a reduced incidence of angiographic restenosis and a reduced need for TLR compared with PES implantation, although incidence of death or myocardial infarction at 9-month follow-up was not significantly different. Our study yielded similar results with SES use being associated with better outcomes than PES use, which might be due to significantly lower late loss (0.4 ± 0.6 mm in SES vs 0.7 ± 0.8 mm in PES, P = 0.007) and TVR rates (2.8% in SES vs 8.5% in PES, P = 0.018). The outcome rates in this study were more favorable than those in the study by Lee et al. (11), which may be secondary to differences in lesion length (mean stent length 71.9 ± 13.7 mm in Lee et al. report (11) vs 45.8 ± 15.5 mm in the present study), because ISR occurrence increases with increased stented length. However, this study was not focused on full lesion coverage such as with full metal jackets, but on the treatment of long lesions more commonly seen in the real-world clinical practice.
Our study showed that MACE of patients with SES had better results in not only efficacy (TLR/TVR) but also myocardial infarction and cardiac death. Compared with the previous reports, our study represented different results in hard endpoints because our data reflected real world clinical practice and long term follow-up for 2 yr in diffuse long coronary artery lesion (13).
From our study, small differences already uncovered before one year follow-up, however the results came to clearer towards two years. This represents short-term follow-up is necessary but also long-term follow-up is important in patients treated with DES, especially PES, in diffuse long lesions.
Stent thrombosis is another important complication in patients treated with DES, especially in diffuse long lesions. One study reported a 9-month late stent thrombosis rate of 1.25% (4/318) for a mean stent length ≥ 55 mm (14). In the present study, 4 stent thrombosis (one acute, two sub-acute and one late) events developed in the PES group (3.4%), while only one subacute stent thrombosis occurred in the SES group (0.5%, P = 0.033). The reasons for this significant difference are unknown and might include multiple factors such as different environmental or individual factors.
There are several limitations in this study. First, angiographic follow-up was performed only in 47.3% of patients, which might underestimate restenosis rates. This could be another major source of selection bias. So we compared between the patients with and without angiographic follow-up. However, there were no differences in baseline characteristics and angiographic, procedural findings. Second, the total number of patients was relatively small to fully assess the safety and efficacy of DES. Third, this study is a retrospective analysis and stent selection was not randomized and could be biased. So we used multivariate regression analysis. From this analysis, used stent and overlapping proved independent risk factors for MACE in patients with diffuse long coronary artery disease as described early. Fourth, another type DES like zotarolimus-eluting stent and second generation DES such as everolimus-eluting stent were not included in this study and further investigation will be warranted.
In conclusion, long-term DES use in diffuse long coronary lesions is associated with favorable results, with SES being more effective and safer than PES in this real-world clinical experience.


 XML Download
XML Download