

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cancer has been the most common cause of death in Korea since 1983, and lung cancer is the leading site among cancer deaths. In 2005, 16,949 new cases of lung cancer occurred in Korea, and the age-standardized incidence rates were 50.2 and 13.2 per 100,000 for males and females, respectively (1). Although its predominant cause is now clearly known to be tobacco smoking, lung cancer is the most common cancer associated with occupational exposures (2). The proportion of lung cancer cases to which occupational exposure contributes is reported to be in the range of 9%-15% (3). In Korea, that was estimated at 7% (4).
In reference to the respiratory cancers, malignant mesothelioma is a well-known occupational cancer caused by asbestos exposure. Malignant mesothelioma is a very rare cancer, and its incidence in Korea was 70-90 new cases per year during 2004-2007 (5-8). However, the mortality rate has increased by more than double in recent years, from 0.4 in 1998 to 0.9/100,000 in 2008 (1). Also, the number of cases detected by a nationwide malignant mesothelioma surveillance system has also increased by nearly three-fold. Thus, Korean society is concerned that a surge of malignant mesothelioma occurrence may begin soon (9, 10). The aim of this review is to overview occupational respiratory cancer including malignant mesothelioma in Korea.
EXPOSURE TO OCCUPATIONAL LUNG CARCINOGENS
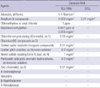
In Korea, 14 agents are listed as carcinogens by the Ministry of Employment and Labor (Table 1) (11). The list is not exactly the same as the list of agents proposed by the International Agency for Research on Cancer (IARC) Group 1. Among those in the former list, carcinogens known to be associated with respiratory cancer include asbestos, bis(choloromethyl)ether, chromium (VI) compound, coaltar pitch volatiles, and nickel compound. In order to use or manufacture these agents, one must obtain permission from the authorities. The manufacturing, import, and use of all kinds of asbestos were banned in 2009.
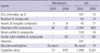
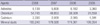
The Korean Occupational Safety and Health Agency (KOSHA) performs the Work Environment Survey every five years. The subjects of this survey are limited to the private sector and include all manufacturers employing more than five workers and some portion of all other companies. Some lung carcinogen-exposed populations were presented in the survey (Table 2) (12). Other useful data include the number of workers who received the special health examination because of exposure to designated hazardous agents (Table 3) (13). The list of agents and the coverage of medical check-ups are specified by law. According to a study using these data, from 2000 to 2004, 2,098 workers were exposed to cokes, and 5,789 to asbestos (14). In a similar study using these data from 2000 to 2002, it was reported that the carcinogenic heavy metal (including arsenic, beryllium, cadmium, chromium, nickel)-exposed population was 32,096 (15).
It shows big gap between the number of exposed workers of Work Environment Survey data and that of Special Health Examination data. Main reason is because Work Environment Survey did not cover small-scale enterprises (less than five workers), public sector and majority of non-manufacturing industry. In case of asbestos, use of any form of asbestos is banned from 2009, but quite many workers are still exposed to asbestos in buildings and facilities. Such exposure due to deconstruction and repair was beyond the scope of Work Environment survey.
COMPENSATION FOR OCCUPATIONAL RESPIRATORY CANCER
Some criteria for granting compensation for occupational diseases are stated in the Enforcement Decree under the Industrial Accident Compensation Insurance (IACI) Act. For example, if primary lung cancer develops in a pneumoconiosis patient whose radiograph defines profusion of 1/0 or greater by the International Labor Organizaion (ILO) classification, the worker will be compensated automatically by this regulation. Another example is asbestos-related diseases. Asbestos-exposed workers who have primary lung cancer or malignant mesothelioma could be compensated if they have asbestosis, signs of asbestos exposure such as pleural plaque, or a history of asbestos exposure for more than 10 yr (16). However, most cases claimed for occupational diseases are evaluated on a case-by-case basis by the Korea Workers' Compensation and Welfare Service (COMWEL), and some of them are investigated in depth by the Occupational Safety and Health Research Institute (OSHRI) in KOSHA to determine whether they are work-related. The official statistics of compensation for occupational injuries and diseases are reported annually by KOSHA. About 10-13 million workers per year were covered by IACI, and the total number of compensated occupational diseases (excluding work-related disease like musculoskeletal, cardiovascular, and cerebrovascular disease) ranged about 2,000-2,500 cases per year in the past five years (17). No data specific to lung cancer or malignant mesothelioma were presented. A number of asbestos related cancer is available since 2006. A few studies have analysed the characteristics of compensated occupational diseases including respiratory cancer using the database of COMWEL; these are summarized as below.
Lung cancer
Ahn et al. (18) analyzed 575 compensated occupational disease cases that occurred in 1999. Among them were 17 cases of cancer, and 11 of these were lung cancer. Six cases of lung cancer were compensated because they were recognized as complications of pneumoconiosis (9). In a similar study of another period using the COMWEL database, Ahn et al. (19) analyzed 4,240 cases of compensated occupational disease that occurred from 2001 to 2003. Sixty-seven cases of lung cancer were approved based on underlying pneumoconiosis, and another 22 lung cancer cases were compensated. Another study collected 120 cases of compensated lung cancer during 1994-2008 (20); cases approved for underlying pneumoconiosis were excluded in their analysis. The number of compensated occupational lung cancer cases increased from 15 during 1994-1999 to 105 cases during 2000-2008. The majority of occupational lung cancers (93.3%) were male. The average age at the time of diagnosis was 51.9 yr, and 63% of the patients were diagnosed in their fifties. The most common pathologic findings were adenocarcinoma (35%), followed by squamous cell carcinoma (19%). The mean duration of occupational exposure was 19.6 yr. The average latency was 21.3 yr, and nearly half of the cases (44.2%) had a latent period of 20-30 yr. The major lung carcinogen was asbestos (45%), followed by hexavalent chromium (30%) and crystalline silica (19%). Prevalent occupations among these cases were welders (14%) and foundry workers (14%), and the rest included painters, platers, plumbers, and vehicle maintenance workers.
Malignant mesothelioma
Ahn et al. (10) analyzed 60 cases of occupational cancer compensated from 1993 to 2007. Among them, 19 cases were malignant mesothelioma. The mean duration of asbestos exposure was 16.0 yr, and the mean latency was 22.6 yr. The types of exposure included the manufacture of asbestos-containing products, use of asbestos-containing products in the manufacturing process, and handling of asbestos-containing products in the course of work. The most common industries related to occupational malignant mesothelioma were shipbuilding and repair (4 cases) and the manufacturing of asbestos textiles (3 cases).
Case investigation by OSHRI
At the request of COMWEL, OSHRI has investigated workers and the workplaces of involved in claims of occupational disease to evaluate work-relatedness since 1992. Cases having a probability of work-relatedness greater than 50% have been recognized as occupational disease. Kang et al. (21) analyzed the data of this investigation from 1992 to 2000. The total number of cancer cases claimed was 108. Fourteen of 46 cases (30.4%) of lung cancer and 6 of 6 cases (100%) of malignant mesothelioma were accepted as occupational cancer. The most common causative agent of lung cancer was asbestos, followed by hexavalent chromium, polycyclic aromatic hydrocarbons (PAHs), and crystalline silica. Asbestos exposure was related to all cases of malignant mesothelioma. Other types of respiratory cancer that have been investigated include laryngeal cancer, nasal cancer, and nasopharyngeal cancer.
OCCUPATIONAL DISEASE SURVEILLANCE SYSTEM
An occupational disease surveillance system have been established to monitor trends in occupational disease and to identify sentinel cases since 1999, supported by OSHRI. In Korea, two types of surveillance systems are used. The first is the regional occupational surveillance system for preventing occupational hazards at the local level. The second is a nation-wide occupational surveillance system for specific target diseases, such as occupational lung cancer, occupational asthma, and malignant mesothelioma.
Occupational Lung Cancer Surveillance System
The Occupational Lung Cancer Surveillance System is a hospital-based system covering nine general hospitals in six regions. The investigators at member hospitals report all cases of first-diagnosed lung cancer in their hospital during a specified period and check the occupational history of the patient. Then, the cases are classified into four groups according to the possibility of work-relatedness: definite, probable, possible, and suspicious. A total of 3,353 cases were reported during 2006-2009, and the number in the definite and probable groups combined was 393 (11.7%). The probable carcinogens to which these patients had been exposed were asbestos (20%), diesel engine exhaust (17%), crystalline silica (14%), and PAHs (10%) (22).
Malignant Mesothelioma Surveillance System
The Mesothelioma Surveillance System began operation in Korea in 2000. When the members of the Korean Society of Pathology confirm malignant mesothelioma, they report it to the surveillance center, and then information about occupational and environmental exposure is collected by telephone interview. Accuracy is the strength of this data because only pathologically confirmed cases are collected. Kim et al. (23) reported that under this system, only 18 cases were reported before 1995, but this increased to 42 in 2004, 37 in 2005, and 53 in 2006 and 55 in 2007. The incidence rate, calculated using the total population of Korea as the denominator, increased rapidly from 0.25 per million in 2001 to 1.14 per million in 2007. The most common occupation among these cases was construction worker, and others included asbestos textile industry workers, welders at a shipbuilding, soldiers, and manufacturing workers. Some patients had histories of environmental exposure, such as residence near a mine or repair the asbestos slate roof of their own house (24, 25).
OCCUPATIONAL RESPIRATORY CANCER RESEARCH
Epidemiological studies
An elevated risk of respiratory cancer among several occupational cohorts was observed. Choi (26) reported that lung cancer was significantly elevated in non-miners with pneumoconiosis (standardized incidence ratio [SIR], 2.6; 95% confidence interval [CI] 1.8-3.8), underground mine workers with pneumoconiosis (SIR, 1.9; 95% CI, 1.8-2.1), and underground mine workers without pneumoconiosis (SIR, 1.9; 95% CI, 1.7-2.2). Based on this result, the criteria for compensation of occupational lung cancer in the IACI. Act were revised in 1999 to compensate primary lung cancer of pneumoconiosis patients with profusion of 1/0 or greater by the ILO classification of pneumoconiosis.
Ahn et al. (27) used the National Health Insurance data to evaluate the risk of lung cancer in foundry workers; a significant positive association was reported between foundry work and the risk of lung cancer (Odds ratio, 10.04; 95% CI, 3.95-25.55; cases=7 foundry workers).
An elevated risk of lung cancer was found among cohorts of male workers exposed to carcinogenic heavy metals including arsenic, beryllium, cadmium, chromium, and nickel, but the association was not significant (SIR, 1.47; 95% CI, 0.67-2.80; cases=9) (15). An analysis of a cohort of carcinogen-exposed workers indicated an excess of lung cancer in asbestos-exposed workers (standardized rate ratio [SRR], 7.87; 95% CI, 1.87-33.15; cases=6 exposed workers) (14).
Kim (28) investigated the occurrence and mortality of malignant mesothelioma and lung cancer among retired workers of a asbestos textile company. Of the 222 subjects, three died of malignant mesothelioma, and six died of lung cancer. An extremely elevated risk of malignant mesothelioma was observed in males (standardized mortality ratio [SMR], 517.1; 95% CI, 130.9-28813.0, case=1) and in females (SMR, 4501.7; 95% CI, 545.2-16262.0; cases=2). The risk of lung cancer was not significantly elevated in males (SMR, 1.4; 95% CI, 0.0-7.6; case=1), but it was significantly elevated in females (SMR, 41.4; 95% CI 13.5-96.7; cases=5).
Although not targeting respiratory cancer, several occupational cohort studies have been conducted to examine the risk of cancer. Park et al. (29) reported no significant association between the iron and steel industry employment and lung cancer (SMR, 0.81; 95% CI, 0.85-2.28; cases=31). Morbidity analysis of the same cohort showed an elevated lung cancer risk among workers in subcontract plants compared with those in parent plants (SRR, 2.35; 95% CI, 1.07-4.92) (30). Non-significant negative associations with lung cancer risk among workers exposed to ionizing radiation were reported in a cohort study (SMR, 0.77; 95% CI, 0.55-1.05; cases=38) (31).
In a study based on patients in one university hospital, 4.6% of primary lung cancer was identified as probable or definite occupational lung cancer, and the presumptive carcinogens included asbestos, heavy metal, inorganic dust, and PAHs (32).
Case reports
In Korea, the first officially reported case of occupational cancer was mesothelioma caused by asbestos exposure in the asbestos textile industry in 1992 (33). This report confirmed high exposure to asbestos associated with a high count of asbestos fiber in pleural tissue. Following that report, lung cancer with pleural asbestosis in a worker exposed to asbestos in manufacturing insulation (34) and malignant pleural mesothelioma in a boilermaker and a plumber (35) were reported in the 1990s. Since 2000, reports have identified lung cancer associated with exposure to coke oven emissions (36), lung cancer in an asbestos-exposed shipyard repairman (37), and lung cancer with silicosis in a plasterer exposed to cement dust contained silica (38).
CONCLUSION
Interest in occupational cancer is growing in Korea. Especially, lung cancer and malignant mesothelioma are well known occupational cancers. We have reviewed the results of scientific articles about compensated occupational respiratory cancer, but the national official statistics did not report the status and trends of compensation for respiratory cancer. Also, a nationwide investigation of the hazardous agent-exposed population was quite limited, so more efforts are needed to estimate the lung carcinogen-exposed population. Few epidemiological studies have examined occupational respiratory cancer, and long-term cohort studies are thus far very limited. Nonetheless, it is expected that more research will be conducted in response to the increasing interest in occupational cancer.
It is difficult to predict the trend for the future incidence of occupational respiratory cancer, but this review demonstrates that occupational respiratory cancer has increased during the last 10 to 20 yr. At present, important programs and regulations are in place to prevent and control occupational cancer, such as banning all forms of asbestos, workplace exposure monitoring, and occupational disease surveillance systems. Indeed, more efforts to advance the systems for the prevention and management of occupational cancer are needed in response to changing technology and work environments.
 XML Download
XML Download