

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Korea started its industrialization since the 1960s and many manufacturing factories were constructed in the 1970s and 1980s. Coal mining increased exponentially to supply the energy to the manufacturing industry and as a home heating source. Various kinds of chemicals have been used in the manufacturing industry. The traditional agriculture has rapidly decreased. Consequently, the transition toward the manufacturing industry led to many traditional occupational diseases such as carbon disulfide and heavy metal poisoning. When the industrialization began, a legal system for workers' compensation was introduced as the first in the Korean social security system. Occupational diseases are covered by the workers' compensation system; however, the system still can miss many unclaimed or unrecognized cases.
The Korea Workers' Compensation and Welfare Service (COMWEL) is a government-affiliated organization responsible for workers' compensation under the Industrial Accident Compensation Insurance (IACI) Act. COMWEL requests the Occupational Safety and Health Research Institute (OSHRI) of the Korea Occupational Safety and Health Agency (KOSHA) to investigate new cases of occupational diseases if there is no clear link between the disease and work. The Ministry of Employment and Labor (MOEL) asks OSHRI to investigate cases of occupational disease if they are new and socially important. OSHRI is also legally supported to investigate workplaces if it is deemed necessary for prevention; as a result, OSHRI examines most new cases of occupational disease in Korea (1).
In this article, authors will discuss the concept of occupational disease and the data resources. We will also describe occupational diseases in Korea based on the review of the cases that OSHRI has investigated, and will add more information from papers published in journals.
DEFINITON AND CLASSIFICATION
Definition of an occupational disease
An occupational disease can be defined as a disease which arises from work or is aggravated by work. The International Labor Organization (ILO) defines occupational disease as a disease contracted as a result of an exposure to risk factors arising from work activity (2). The World Health Organization (WHO) states that an occupational disease is not characterized merely by the disease itself, but by a combination of a disease and an exposure, as well as an association between the two parts (3).
The term occupational disease can be academic, which means that an occupational disease is defined regardless of compensation. However, the term occupational disease generally means a disease arising from work that is to be compensated through insurance or a fund contributed to by the employers. The extent of the compensation relies on the coverage of workers' compensation insurance. In Korea, only paid employees are subject to compensation for occupational disease under the term of 'disease due to business' with IACI Act.
Classification of occupational disease
An occupational disease is usually compensated through Workers' Compensation Insurance or Social Security Fund in most countries because employers are responsible for such occurrence. Conditions for compensation are different in each country that may exceed the list of 106 occupational diseases with 4 categories by the ILO Recommendation 194 adopted in 2002 and amended in 2010 (4). Korea compensates occupational diseases as 'disease due to business' that includes cerebro-cardiovascular diseases (CVDs); the extent of which is beyond the ILO recommendation.
For the prevention purpose, 'disease due to business' is classified into two categories that depend on work relatedness. One is traditional occupational diseases that can be caused only by occupational reason. They are diseases from exposure to chemicals, physical environment and biological agents. The other is work-related diseases that can be aggravated, triggered or influenced by working conditions. They are musculoskeletal diseases (MSDs) or CVDs that are caused by multiple causal factors including occupational fraction. However, the term occupational disease is also used to express 'diseases due to business' in general, hence occupational diseases, hereafter, means 'diseases due to business'.
RESOURCES ON OCCUPATIONAL DISEASE DATA
In Korea, a claim for compensation for occupational diseases requires more than 3 days of treatment. The MOEL has published statistics on occupational diseases based on compensated cases. The statistics on occupational diseases includes the diseases for all paid employees except government officers, private school teachers, and self-employed workers (including farmers). In 2009, the IACI covered 13.9 million workers, which represents 57.2% of the economically active population (24.3 million), or 86.2% of wage earners (16.1 million).
There are several sources that provide the information on occupational disease. The official statistics come from compensation data of COMWEL, that also sends the information on compensated cases to KOSHA electronically. KOSHA analyses the data and submits the report on the official statistics for occupational diseases to the MOEL. Supplemental information can be provided by the periodic Special Health Examination (SHE), the Occupational Disease Surveillance System, case reports or investigations from scientific journals.
Limited cases are claimed for compensation although all paid workers are mandatorily engaged in the coverage of workers compensation, regardless of employers' payment status of insurance premiums. However, many cases for compensation are not made because it is difficult for most clinicians as well as workers to recognize occupational diseases. Furthermore workers who have non-serious occupational diseases that usually require only simple medical treatment (such as dermatitis) are not willing to claim compensation because they are afraid of unwanted trouble with employers.
Compensation by the Industrial Accident Compensation Insurance
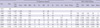
Statistics for occupational diseases are available since 1979 while data for all compensated cases are available since 1964 (5). A separate data for specific diseases are available since 1991, because the Occupational Safety and Health (OSH) Act was completely amended in 1990. Occupational diseases and work-related diseases were separated since 1996. Fatal cases have been reported separately since 1998. In 2003, the acceptance criterion of pneumoconiosis was amended toward to be expanded. CVDs have been separated into cerebrovascular and cardiovascular diseases since 2003. In 2006, back pain that occurred accidentally was classified into work-related diseases from injuries and since then more detailed information in classification has been provided. The diagnostic criterion for CVDs was amended to be strict in 2008 (Table 1).
Special Health Examination
The results of the SHE also provide some information on occupational diseases status. It gives good information on asymptomatic diseases with positive findings such as pneumoconiosis and noise-induced hearing loss (NIHL). More than 95% of positive results by the SHE were one of them. The SHE also detects chronic poisoning caused by chemicals for which biological monitoring is available.
Occupational Disease Surveillance
OSHRI has financially supported academia to conduct a surveillance program to capture occupational diseases that were usually missing in official statistics since 2000. The surveillance program consists of two types: regional based programs and disease specific programs. Disease specific programs that focus on occupational asthma (6, 7) or mesothelioma (8) are being successfully operated. The programs were successful because allergists and pathologists work together with occupational physicians through regular academic conferences. They capture unclaimed cases for compensation that were not included in the national statistics as well as claimed cases.
COMEPENSATION PROCESS
The process of compensation
A worker who has an occupational disease can be compensated regardless of payment of premium by employers, because joining the IACI is a mandatory requirement for all enterprises. A worker can make a claim for compensation to COMWEL with a medical diagnosis from any physician in order to be approved as an occupational disease. The local office of COMWEL requests the case to the Committee on Occupational Diseases Judgment (CODJ) of the Regional Office unless it is pneumoconiosis or carbon disulfide poisoning, or a case of which the causal relationship is clear. The committee is composed of lawyers or labor consultants, professors, physicians or dentists and persons who have experience in compensation more than 5 yr. At least one third of the members of the committee should be experts, recommended by employers' association and trade union. The worker can appeal to the IACI Examination Committee if the claim is rejected.
If the appeal is not accepted, they can re-appeal to the IACI Reexamination Committee (which is independent from COMWEL) and appointed by the President of the Republic of Korea. Finally, workers can file a lawsuit against COMWEL. Workers can go directly to the court without appealing to the Examination or Reexamination Committee.
If COMWEL or CODJ faces trouble in judging the case, they can ask OSHRI to investigate it. OSHRI investigates the case through workplace visit and medical evaluation to report its professional opinion about the causal relationship. OSHRI also has an expert committee, the Committee on Evaluation of Epidemiologic Investigation, which consists of occupational physicians and industrial hygienists.
Diagnostic criteria
Korea has a prescribed list of occupational diseases. The Presidential Decree of Labor Standard Act (9) stipulates 38 prescribed diseases. The 38th clause in the list is any disease in which the causal relationship to work is clear. With this clause, any disease can be accepted as an occupational disease if there is sufficient evidence of work-relatedness by the investigation. The detailed diagnostic criteria for 23 occupational diseases are provided in the Presidential Decree of IACI Act (10). The act includes the diagnostic criteria for work-related musculoskeletal disorders (WR-MSD), work-related cerebro-cardiovascular diseases (WR-CVD) and liver disease that are not found in most European countries.
Compensated occupational diseases
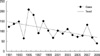
The total number of compensated occupational disease cases from 1972 to 2009 (including fatal cases) was 119,713. Fatal cases were usually counted twice, unless the victims had already died before their claim was accepted. Before 1991, most cases of occupational diseases were pneumoconiosis. From 1991, the proportion of pneumoconiosis was 67.1% among occupational diseases, and NIHL and diseases caused by chemicals were 16.1%, and 7.2%, respectively (11). Pneumoconiosis had continuously decreased by 2001 but there was a sharp increase in 2003 when the diagnostic criterion was expanded to include mild cases. The number of NIHL is constant at approximately 200 cases a year. Diseases caused by chemicals are continuously decreasing (Fig. 1). Recently, occupational infectious diseases have increased. Work-related diseases including WR-CVDs and WR-MSDs have increased since 1996 after the diagnostic criteria for those diseases were established. From 1996 to 2009, back pain accounted for 41.2% of work-related diseases, followed by WR-CVD at 30.3% and WR-MSD (excluding back pain) at 25.2%.
OCCUPATIONAL DISEASES IN KOREA
Occupational diseases caused by exposure to agents arising from work activities
Diseases caused by chemical agents
Lead poisoning has been the most common occupational diseases caused by chemicals. An outbreak of lead poisoning was clustered around storage battery workers in 1982. The blood lead level was more than 40 µg/dL in 75% of the total 234 workers (12). Workers with lead poisoning showed anemia, neurologic diseases (13), renal dysfunction (14), and neurobehavioral changes (15). Since 2000, less than 5 cases whose blood lead level exceeds 40 µg/dL, have been reported.
Nasal septal perforation was found in plating workers exposed to chromium mist. In 1988, the prevalence rates of nasal septal perforation and ulceration of mucosa of the plating workers were 31.7% and 10.5%, respectively out of 627 workers, according to a cross-sectional study (16). Since the late 1990s, nasal septal perforations are rarely found. Nasal septal perforations were also found in welders who were exposed to welding fumes that included hexa-valent chromium (17).
Mercury poisoning occurred in the thermometer and fluorescent lamp manufacturing industry in the early 1990s (18). There was a debate over the possibility of cadmium poisoning in a worker who worked in a zinc galvanizing factory (19). After then, there were many cases of misdiagnosed cadmium poisoning because of the low quality of analyzing biological samples. Hence, the quality control program for biological monitoring was adopted in 1995 (20). Proteinuria was found in workers at a cadmium smelting factory and battery recycling factory; a renal biopsy subsequently showed interstitial fibrosis (21).
The first report of manganese poisoning were attributed to ore crushing work (22). Increasing signal intensity in Magnetic Resonance Imaging (MRI) was found in welders (23). Some cases of Parkinson syndrome due to manganese exposure in welders were accepted for compensation; however, increased signal intensity does not necessarily translate into manganese poisoning (24). The Pallidal index on MRI is the most effective predictor of neurobehavioral performance in workers exposed to manganese because it reflects the target organ dose of occupational manganese exposure (25). Signal intensity on MRI is an effective predictor of the neurobehavioral performance of manganese exposed workers (26).
The outbreak of carbon disulfide poisoning (27) in the early 1990s was the most serious occupational disease in Korea, which eventually led to approximately 1,000 cases of compensation by 2009. The signs of carbon disulfide poisoning were retinal microaneurysm (28), renal glomerulosclerosis (29), multiple cerebral infarction (30), peripheral neuropathy (31), ischemic heart disease, mental diseases, impotence (32), etc.
Various health effects caused by organic solvents have been reported (33). They are demyelinating lesion of the brain by toluene based solvents (34), neurologic diseases by acetonitrile, peripheral neuropathy by acrylamide (35), temporary strabismus by optic nerve palsy by phosphorus trioxide, cerebellar ataxia by mixed solvents, amyotrophic lateral sclerosis by solvents and metals (36), Mobitz type 2 ventricular bundle branch block by toluene based organic solvents, premature ventricular beats caused by trichloroethylene, and cardiomyopathy by carbon monoxide. Bone marrow suppression by ethylene glycol monoethyl ether acetates was found in painters at a shipyard (37). Neurologic diseases caused by methyl bromide were found in fumigation workers (38, 39). Workers exposed to methyl bromide showed high signal intensities in the medulla oblongata and paravermian of cerebellum in MRI or polyneuropathy in a nerve conduction velocity study.
In 1995, reproductive problems were reported for the first time in workers exposed to 2-bromoprophane at an electronic supplier factory (40). The workers were exposed to a level exceeding the occupational exposure level of Korea.
Toxic hepatitis occurred in workers exposed to dimethylformamide, which is used to produce synthetic fiber or synthetic leather (41). Several cases of toxic hepatitis developed to fatal fulminant hepatitis (42, 43). Toxic hepatitis occurs usually within 2-4 weeks after exposure. A liver function test is mandatorily performed on workers who are newly engaged to work of being exposed to diemthylformamide, within 4 weeks of the initial assignment to the task. Severe toxic hepatitis with erythematous skin diseases caused by trichloroethylene were reported (44-46).
In 2005, 8 Thai migrant workers developed peripheral neuropathy. They were exposed to 150-200 ppm of n-hexane (47). Peripheral neuropathy by n-hexane is continuously reported in the IT industry (48) because it is non-irritant and easily removes blemishes from plastic products.
OSHRI reported conjunctivitis by chlorine in a worker at a swimming pool, conjunctivitis by organic solvents, acid and alkali, naso-lachrymal duct obstruction by resin dust, and macular degeneration by methanol. Macular degeneration was also reported in welders (49).
Diseases caused by physical agents
NIHL is the second common occupational diseases. Annually 200-300 cases are compensated. Sudden hearing loss was reported after exposure to high level of noise (50). Approximately 10 cases of disease by vibration are compensated in a year. Handarm vibration syndrome was reported in workers using a grinder that produced hand transmitted vibration (51, 52). Heat related diseases such as heat stroke were also reported (53). Diseases caused by compressed or decompressed air (54, 55) have been continuously reported.
Biological agents and infectious or parasitic diseases
Occupational infectious diseases increased. In 2009, the number increased to 427 cases, which was 3 times more than that of 2008. They were mostly tsutsugamushi disease which occurred among public service laborers who performed landscape gardening (56). Tuberculosis is a common infectious disease among health care workers (57, 58). Seroconverted viral hepatitis after needle stick injury among health care workers is generally accepted as occupational disease although their seroprevalence rates were not different from those of the general population (59).
Although farmers are not included in the IACI, brucellosis can be found among farmers (60).
Occupational diseases by target organ systems
Respiratory diseases
The most common occupational respiratory disease is coal workers' pneumoconiosis that occurs most often in coalminers. The amount of compensated cases of pneumoconiosis from 1991 to 2009 were 19,127. However, the total cases of pneumoconiosis since 1972 could be approximately 40,000 if we consider the 24,754 cases from 1972 to 1990 when more than 95% of compensated cases were pneumoconiosis. The compensated cases of fatality by pneumoconiosis from 1998 to 2009 were 4,864. The case of pneumoconiosis will continue to decrease as most mines were closed in the early 1990s and only several mines are active as of 2010. Tuberculosis, emphysema, bronchitis, bronchiectasis, and cor-pulmonale accompanying with pneumoconiosis are also conditions that can be compensated for. Pneumoconiosis is also reported by welders (61) and foundry workers (62).
Occupational asthma is the second most common occupational respiratory disease in Korea. Toluene diisocyanate (TDI) (63, 64) is the most common causative agent followed by reactive dyes (65). Occupational asthma caused by various agents such as chromium (66), antibiotics and digestives (67), latex (68), grain dust (69), flour (70), and citrus red mite in citrus farmers (71) were also reported. Occupational asthma caused by colophony is rarely reported even though it is one of the most common causative agents in the UK.
OSHRI reported metal fume fever by zinc fume, chronic obstructive lung diseases by waste materials, hypersensitivity by TDI, idiopathic interstitial lung disease by styrene, eosinophilic pneumonia by nickel, acute respiratory failure in a welder, and diffuse interstitial lung diseases by organic solvents.
Skin diseases
Occupational dermatitis is a common workplaces problem (72), but rarely reported because it is not a serious disease. Most skin diseases were contact dermatitis, vitiligo by hydroquinone, and dermal pigmentation by 2,5 hexandione (73). Contact dermatitis, chloroacne, chemical burns by fluoric acid, and hand eczema were common in the semiconductor industry (74).
Musculoskeletal disorders
WR-MSDs were first reported in the late 1980s in telecommunication workers (75, 76). Since then, many cases of WR-MSD were claimed; most of which were attributed to the assembly processes in the manufacturing industry and they were expanded to the service industry. In 1998, records from a university hospital showed that 34.7% of carpal tunnel syndrome were work-related; however, less than 1% filed for compensation (77). The occupation of patients were various and included restaurant workers, assemblers, manual workers, farmers, fishermen, health care workers, and construction laborers. In 2005 according to analysis for the cause of occupational diseases (78), 73.9% of MSD excluding back pain cases were reported in the manufacturing industry. The main cause of MSD was due to awkward position (50.2%), strenuous forces (28.2%), and repetitive work (16.8%).
The number of occupational back pain disorders has changed widely depending on the classification system. Occupational back pain was mostly classified as an accidental injury because workers usually described the onset of symptoms as abrupt. These cases have been included in occupational diseases since 2006. Herniated intervertebral disc was the major back pain disease (67.5%).
Mental and behavioral disorders
Stress related mental disorder can be accepted as occupational diseases. Post-traumatic stress disorder can develop after a serious industrial accident (79). Conductors of underground subway trains have experienced panic disorder after serious train-passenger accidents (80). Under special conditions, suicide by workers who have a confirmed mental disorder (such as depression) can be compensated.
Occupational cancer
In 1997, the number of occupational cancer was estimated from 32-56 cases a year (81). Recently the attributable risk of occupational cancer was calculated at 1.1%, which was lower than that reported in developed countries (82).
Compensated occupational cancers were mesothelioma, and lung cancer by asbestos, leukemia by benzene, and lung cancer by crystalline silica (83). The first case of bladder cancer caused by benzidine-based dye was reported in 1999 (84). Bladder cancers are very rare, because Korea did not use benzidine and 2-naphthylamine when it started to produce dyes in the 1970s. Since 2002, primary lung cancer with pneumoconiosis is also compensable condition because coal produced in Korea contained 5%-10% of crystalline silica and the risk of lung cancer increased in pneumoconiosis patients (85).
Hepatoma is sometimes accepted by the court to be an occupational disease under the assumption that stress or long working hours could aggravate or trigger the development of hepatoma in workers who have viral hepatitis B.
Asbestos
The first case of mesothelioma caused by asbestos was found in a female worker in an asbestos textile factory in 1993 (86). Since 1972, asbestos was widely used after Korea changed roofs from rice sheaves to asbestos corrugated roofing slates. The total amount of asbestos use was estimated at 2,026,963 tons (87). The annual cases of mesothelioma are approximately 40 to 50 in Korea and continuously increasing (88); however, few cases were accepted as occupational cancer (83). The incidence of mesothelioma remains relatively low compared to other industrialized countries and it may be caused by delayed peak period of consumption. However, another reason would be the different way of use - in the case of Korea, asbestos was rarely used in spraying and for thermal insulation.
Benzene
Benzene was not used in Korea for manufacturing glue because of the late industrialization. Glue, adhesive, and solvents that contained mainly toluene were widely used. However, solvent based chemicals contain benzene as an impurity. The first cancer caused by benzene (officially recognized in 1998) was myeloid dysplastic syndrome of a worker at a tire manufacturing factory, who used adhesives that contained benzene as an impurity (89). After that, many cases of leukemia were reported in different industries (90). In 2000, it was estimated that 200,000 workers could be exposed to benzene at work, which meant that many cases of benzene induced leukemia could have occurred. Recently, leukemia cases that occurred in the semiconductor industry have gained public attention. However, there was no convincing evidence of an increased incidence of leukemia in the semiconductor industry by the epidemiologic investigation performed by OSHRI (91).
Other diseases
Cerebro-cardiovascular disease
CVD was compensated as an occupational disease since 1994 when its diagnostic criterion was established (amended in 2008). Two conditions are required to be accepted as WR-CVD. One is a disease entity and the other is pre-existed working condition such as long working hours or job stress.
This diagnostic criterion of work-related CVD was established due to social pressure. CVD was not on the list when the IACI Act was established in 1963. Most cases of claimed CVD were not accepted as work-related, which led many workers and relatives to go to the courts in the early 1990s. The court accepted CVD as work-related if the workers proved that they suffered from long working hours or job stress. Consequently, the diagnostic criteria for work-related diseases expanded in 1994 and WR-CVD cases have rapidly increased due to the generous application procedure in conjunction with the increased workload after the economic crisis in 1998.
From 1996 to 2009, 20,143 cases were accepted as WR-CVD. The number of compensated cases peaked in 2003 and gradually decreased due of active prevention activities for life-style diseases such as hypertension or hyperlipidemia at workplaces. The number of compensated cases has sharply decreased since 2008, after amendments of the diagnostic criterion. In 2008, the expenses for CVD accounted for 9.5% of total expenses for compensation.
SUMMARY
Since the 1990s most chemical related diseases and pneumoconiosis have rapidly decreased by improving work environment. However, careful attention is needed because unexpected chemical poisoning occurred continuously in the past, and occupational cancers are increasing. Since 2000, the characteristics of compensated occupational diseases of Korea became distinct from that of many European countries because Korea compensates cerebro-cardiovascular diseases as work-related and is generous in musculoskeletal diseases compensation.
 XML Download
XML Download