

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hepatitis B virus e antigen (HBeAg) negative chronic hepatitis B (CHB) represents a late phase of chronic hepatitis B virus (HBV) infection usually caused by precore or basic core promoter mutant viruses that are unable to produce HBeAg (1). HBeAg negative CHB is predominantly found in the Mediterranean region and Southern Europe, the middle East, and Asian countries, including Korea (2, 3). The prevalence of precore mutants varies geographically and is affected by the HBV genotype. In North Europe and North America, where genotype A predominates, HBeAg negative CHB is rare because cytosine at position 1858 (C-1858) precludes the selection of G1896A precore mutation. In Korea almost all patients with CHB have genotype C and both precore mutant and basic core promoter mutant are very common (3-5).
HBeAg negative CHB is a potentially severe and progressive form of liver disease with rare spontaneous remission and a high risk of progression to liver cirrhosis (6, 7). Moreover, it is harder to induce long-term sustained responsiveness after antiviral therapy in HBeAg negative CHB patients. A sustained-off therapy response rate has been reported at 10-30% in response to conventional interferon-α therapy (2, 8). Therefore, oral nucleos(t)ide analogues have been primarily considered, and used as, a therapeutic for HBeAg negative CHB.
Lamivudine is the first oral nucleoside analogue that has been used in the treatment of patients with HBeAg negative CHB. Therapy for 1 yr achieves complete (both biochemical and virological) responses at the end of therapy in approximately 2/3 of the patients (9-13). However, relapse after withdrawal of lamivudine is universal in patients who were treated for only 1 yr (14). Long-term maintenance therapy with lamivudine has been tried, but the response rate decreases with time because of the increasing emergence of lamivudine resistant mutants (9, 11, 12, 15). Most hepatitis B guidelines suggest that HBeAg negative CHB should be treated with oral nucleos(t)ide analogues for more than 1 yr, yet fail to address the duration of oral nucleos(t)ide analogues therapy beyond the first year (16-18). American Association for the Study of Liver Disease (AASLD) guideline suggest that treatment should be continued until the patient has achieved HBsAg clearance (16). However, long-term nucleos(t)ide analogue therapy has the potential risk of developing resistance or drug toxicity. In this study, we prospectively investigated the clinical efficacy of a 24-months course of lamivudine therapy in patients with HBeAg negative CHB.
MATERIALS AND METHODS
Patients and design of study
This prospective study included a total of 50 patients with HBeAg negative CHB who started lamivudine therapy between December 1997 and December 2004 at Gangnam Severance Hospital in Korea. Over the course of 24 months, 100 mg of lamivudine was administered to patients daily. Patients who showed complete response at 24 months were removed from lamivudine therapy and had regular follow-up. Lamivudine therapy continued in patients who did not show complete response at 24 months. Patient followed-up consisted of physical examination, a routine laboratory test at least every 3 months, and an HBV DNA test at least every 6 months to check for any breakthrough. Complete response was defined as both normalization of alanine aminotransferase (ALT) and undetectability of HBV DNA (<0.5 pg/mL) according to hybrid capture assay.
Inclusion criteria was as follows: 1) Hepatitis B surface antigen (HBsAg) positive and HBeAg negative for longer than 6 months; 2) ALT elevation >1.5 of the upper limit of normal levels and HBV DNA positive within one month of the study; 3) No history of previous antiviral therapy; and 4) No interferon-α treatment within 18 months before the enrollment. No patients were positive to anti-hepatitis C virus (HCV) antibody (Ab) or anti-human immunodeficiency virus (HIV) Ab. Patients who had decompensated liver disease or hepatocellular carcinoma were excluded. This study was approved by the institutional review board (IRB approval number: 3-2007-0060) at Gangnam Severance Hospital (Seoul, Korea), and all participants gave written, informed consent.
HBV serological markers
HBsAg and HBeAg/Ab were determined by enzyme immunoassay (Dade Behring, Marburg, Germany). HBV DNA was measured by Digene hybrid capture assay (Digene Diagnostics, Beltsville, MD, USA) with a lower limit of 0.5 pg/mL. The antibody against HCV was detected by a third-generation enzyme-linked immunosorbent assay (Korea Greencross, Yongin, Korea).
Statistics
All data were analyzed using the statistical software SPSS (version 11.0, SPSS Inc., Chicago, IL, USA). Quantitative variables are expressed as mean±standard deviation. Data were analyzed using Student's t-test, Mann-Whitney U test, and the chi-square test. The Kaplan-Meier method was used to estimate the durability of response after stopping lamivudine therapy. Data were considered to be statistically significant with P<0.05.
RESULTS
Baseline characteristics
The baseline characteristics of the 50 patients are presented in Table 1. There were 39 men and 11 women, with a mean age of 43±11 yr. Median serum AST and ALT levels were 152 IU/L and 239 IU/L, respectively. All patients were HBV DNA positive (>0.5 pg/mL). Fifteen patients (30%) were clinically diagnosed with liver cirrhosis. Twelve patients (24%) had a history of previous interferon-α therapy. Thirty six patients (72%) had a family history of HBV infection. The total follow-up duration from the beginning of lamivudine therapy was 64.7±22.5 (range, 36-120) months.
Response and clinical breakthrough during a 24 months-course of lamivudine therapy
Complete response was defined as having both ALT normalization and HBV DNA undetectability (<0.5 pg/mL) as measured by the hybrid capture assay. The complete response rate at 3, 6, 12, and 24 months of lamivudine therapy was 64.0% (32 of 50 patients), 90.0% (45 of 50), 86.0% (43 of 50), and 86.0% (43 of 50), respectively (Fig. 1). Cumulative clinical breakthrough (HBV DNA positive conversion with ALT re-elevation) occurred in 4.0% (2 of 50 patients) at 12 months, and 14.0% (7 of 50 patients) at 24 months of therapy (Fig. 1). Lamivudine therapy was stopped in 43 patients who showed complete response at the end of 24 months. Among the 7 patients who did not show complete response at the end of 24 months, 2 patients continued lamivudine therapy and the other 5 patients switched to adefovir therapy.
Durability of response after cessation of lamivudine therapy
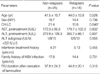
The 43 patients who showed complete response without evidence of clinical breakthrough at 24 months of lamivudine therapy were removed from treatment and regular follow-up was done thereafter. In these patients, the mean duration of follow-up after cessation of lamivudine therapy was 40.8±22.7 (range 12-96) months. The number of patients at follow up months 12, 24, 36, 48, and 60 were 33, 18, 14, 8, and 5, respectively. The expected durability of response after cessation of 24 months-course lamivudine therapy was calculated by the Kaplan-Meier method, and the results at months 12, 24, 36, 48, and 60 of follow-up were 79.1%, 64.0%, 56.9%, 47.4%, and 47.4%, respectively (Fig. 2). There were no episodes of hepatic decompensation in relapsed patients after withdrawal of lamivudine. When comparing the characteristics of those who have relapsed and those who have not relapsed, the proportion of liver cirrhosis patients was significantly higher in relapsers than non-relapsers (44% vs. 16%, P=0.040). Meanwhile, there was no difference in age, sex, baseline ALT level, previous interferon treatment history, family history of hepatitis B, or the follow-up duration after cessation of lamivudine therapy between the two groups (Table 2).
Response during lamivudine re-treatment in relapsed patients after cessation of lamivudine therapy
Fourteen patients among 18 patients who relapsed after cessation of lamivudine therapy were retreated with lamivudine. Complete response rates at 3, 6, 12, 18, and 24 months of lamivudine re-treatment were 64.2% (9 of 14 patients), 92.8% (13 of 14 patients), 100.0% (14 of 14 patients), 83.3% (10 of 12 patients), 70.0% (7 of 10 patients), respectively (Fig. 3). Clinical breakthrough (HBV DNA positive conversion with ALT re-elevation) occurred in 30.0% of patients during the second year of the re-treatment period (Fig. 3). The flow chart of the 24-months course of lamivudine therapy in HBeAg negative CHB patients is illustrated in Fig. 4.
DISCUSSION
Lamivudine has been widely used as an initial antiviral agent for the treatment of patients with chronic hepatitis B. Although there have been recent developments of anti-viral agents with a lower probability of viral resistance, such as adefovir or entecavir, lamivudine is still being widely used due to relatively cheap cost, rapid action, and proven safety for long-term use. Lamivudine monotherapy has been shown to benefit patients with HBeAg positive- or HBeAg negative-CHB (12, 19). For HBeAg positive CHB, HBeAg loss or seroconversion has been used as an indicator for considering when to stop oral antiviral therapy (16-18). According to AASLD practice guidelines, lamivudine therapy should be continued at least 6 months after the achievement of HBeAg seroconversion (16).
However, there is no indicator to determine treatment duration in HBeAg negative CHB patients. The optimal duration of treatment in HBeAg negative CHB is unknown. One year treatment with lamivudine in HBeAg negative CHB patients resulted in HBV DNA suppression to undetectable levels by PCR in 60 to 70% of patients (9-13). Most patients relapsed after withdrawal of lamivudine after 1 yr of treatment (14). This result supports the rationale that most practice guidelines recommend prolonged oral nucleos(t)ide analogue treatment for a period exceeding 1 yr in patients with HBeAg negative CHB (16-18).
Several prolonged antiviral therapies, for periods longer than 1 yr, have been tried in HBeAg negative CHB patients. Virological and biochemical response rates peaked at 12 months and decreased thereafter (9-13). It was reported that virological remission rates at years 1, 2, and 3 were 77%, 52%, and 42%, respectively, in Greek patients with HBeAg negative CHB. HBV genotype D is predominant in Greece, and almost all patients had HBV with precore stop codon mutation (11). Another study conducted in Greece reported that the virological response rate during the second year of lamivudine therapy in HBeAg negative patients was 34% (12). Long-term therapy with lamivudine in HBeAg negative CHB patients in the Mediterranean region, has been associated with increasing rates of virological breakthrough due to the selection of mutants of the YMDD motif of HBV DNA polymerase gene (rtM204I/V±rtL180M) (9, 11, 12, 15). Therefore, the decision to continue oral nucleos(t)ide therapy beyond 1 yr in HBeAg negative CHB should weigh the likelihood of benefit against the risk of developing resistance or drug toxicity (17).
There are two intriguing reports that confine the duration of antiviral therapy to two years in HBeAg negative CHB patients (20, 21). A study with a limited number of patients conducted in Spain, in which most patients had genotype A or D, showed that the response rates at years 1 and 2 of limivudine therapy were 81% and 69% respectively (20). Another study conducted in Canada reported that HBV DNA undetectability rates at years 1 and 2 of treatment were 92% and 86%, respectively, according to the hybrid capture assay during the 2-yr course of lamivudine therapy in 50 Chinese patients with HBeAg negative CHB. Most patients in the study had the HBV genotype C (21). The expected durability rates of virological response at 6, 12, and 18 months were 70%, 50%, and 50%, respectively (21).
Our results showed that the initial response rate at years 1 and 2 of lamivudine therapy was 86.0% and 86.0%, respectively, which compare well with those of a previous study by Fung et al. (21). Unlike previous reports in the Mediterranean region that show initial response rates during the first year of therapy dramatically fall during the second year, our study indicated that the initial response rate of the first year nearly maintained until the end of the second year of lamivudine treatment in Korean patients. Furthermore, our data indicated that the emergence rates of clinical breakthrough due to viral resistance during years 1 and 2 of lamivudine therapy were 4.0% and 14.0%, respectively, a rate lower than those reported in Southern Europe (9, 11, 12, 15). Lok et al. (22) reported that lamivudine resistant mutants were detected at similar rates in both patients with HBeAg positive CHB and those with HBeAg negative CHB. However, previous reports conducted in Asia, including Hong Kong and Korea, reported that the viral breakthrough rate was lower in HBeAg negative CHB patients than HBeAg positive CHB patients during long-term lamivudine therapy (23-25).
The differences of virological factors, including HBV genotype and the prevalence of precore or core promoter mutations, between Southern Europeans and Koreans may contribute to a difference in responsiveness to anti-viral therapy in HBeAg negative CHB. Although we did not analyze HBV genotypes or precore/core promoter mutations in this study, previous reports demonstrate that almost all Korean patients with chronic hepatitis B have genotype C and both precore mutant and basic core promoter mutants are very common in HBeAg negative CHB patients in Korea (3-5). Lamivudine therapy resulted in transient reversion to wild-type HBV from precore/core promoter mutants in Korea (26), but these changes were not observed in a long-term study of Greek patients treated with lamivudine (9). As the precore and core promoter mutants decrease or abolish HBeAg excretion and increase replication capacity (27, 28), the transient reversion to wild type precore/core promoter HBV, during lamivudine therapy in Korean HBeAg negative CHB patients, may delay the emergence of lamivudine-resistant mutant HBV in Korea. However, further studies will be needed to investigate the mechanism of the low rate of lamivudine resistance in Korean patients with HBeAg negative CHB.
Our data showed that the expected off-treament durability at months 12, 24, and 36 of follow-up in complete responders after a 24-months course of lamivudine therapy was 79.1%, 64.0%, and 56.9%, respectively. Most patients who relapsed after cessation of lamivudine therapy occurred within 24 months and then reached a plateau after 48 months of withdrawal from lamivudine therapy. Our data indicate that a 24-months course of lamivudine therapy could induce long-term remission in approximately half of the patients with HBeAg negative CHB in Korea, suggesting a 24-months course of lamivudine therapy could be a feasible option as a first line therapeutic strategy in the treatment of HBeAg negative CHB in Korean patients. When we compared the characteristics of relapsers and non-relapsers, the proportion of liver cirrhosis was significantly higher in relapsers than non-relapsers, suggesting cirrhotic patients with HBeAg negative CHB may require prolonged treatment (16-18). Of the patients who relapsed after withdrawal from lamivudine, none developed hepatic decompensation. Those patients who relapsed after withdrawal from lamivudine therapy were re-treated. Interestingly, the patient response to re-treatment was substantial. Nearly all patients showed ALT normalization with HBV DNA undetectability at 1 yr after re-treatment with lamivudine.
Our study had several limitations. The number of patients included was relatively small, and HBV DNA was measured by the hybrid capture assay, which is less sensitive than a PCR-based assay. However, those limitations could not be overcome in this study because the study was designed and started as a long-term prospective study from the late 1990s when HBV DNA quantitation by PCR was not routinely used in clinical setting. Based upon our data, a larger scaled study adopting more sensitive HBV DNA quantitation method would be necessary in the future.
In conclusion, A 24-months course of lamivudine therapy in Korean patients shows a significant initial response rate, and long-term remission can be maintained in about half of complete responders at 24-months after withdrawal of lamivudine. Moreover, lamivudine re-treatment is still effective in the viral suppression in relapsers after cessation of lamivudine therapy. Therefore a 24-months course of lamivudine therapy may be a feasible option as a first line therapeutic strategy in the treatment of HBeAg negative CHB in Korean patients.





 XML Download
XML Download