

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Since the successful development of methods for islet transplantation (1) through the portal vein, the liver has become the most widely used islet implantation site in clinical trials. However, doubts have been raised about the liver as an ideal islet transplantation site because of complications associated with intraportal islet infusion, such as bleeding and thrombosis (2), low efficiency because of the primary loss of the functional islet mass by an immediate blood-mediated inflammatory reaction (3), impossibility of graft retrieval (4), and progressive deterioration of intrahepatic islet function (5) due to the failure of engraftment.
Numerous sites have been investigated as an ideal islet implantation site, including the kidney subcapsule (6, 7), liver (6-8), peritoneum (8, 9) omental pouch (10), skeletal muscle (9, 11), subcutaneous tissue (8, 11), and spleen (6). However, it is difficult to determine the ideal implantation site based on these published data because of the variety of donor islets (fetal islet-like clusters vs. adult islets), the species of donor and recipients (rat, mouse, and pig), the parameters used to determine the success of implantation (metabolic control, oxygen tension, or functional mass) and the number of sites compared. In addition, no study has considered the operative feasibility, which could affect the success rate of the transplantation. A study comparing the numerous implantation sites using the same strain as the donor and recipient and the same parameters evaluated by a single operator to assess the success rate would provide more practical information for determining the ideal islet implantation site.
To identify the optimal site for islet implantation, we assessed operative feasibility, implantation efficiency, and glycemic control efficiency and compared these between islets transplanted into four sites including the kidney subcapsule, liver, muscle, and omental pouch, which are the most favourable sites for engraftment. The pancreatic islets isolated from C57BL/6 mice were transplanted syngeneically into a group of inbred streptozotocin-induced diabetic recipients at each of the four sites. The operative time and mortality rate were measured to assess operative feasibility. The implantation efficiency was measured as the marginal mass that cured hyperglycemia, and the mean time to reach euglycemia. The glycemic control efficiency was measured using an intraperitoneal glucose tolerance test (IPGTT).
MATERIALS AND METHODS
Mice
Male inbred C57BL/6 mice, aged 9 to 11 weeks, were used as islet donors and recipients. All mice were obtained from Korea Animal Technology (Koatech Inc., Seoul, Korea) and maintained in the Seoul National University SPF animal facilities. The experimental protocols were approved by the Institutional Animal Care and Use Committee. Diabetes was induced by the intraperitoneal (IP) injection of streptozotocin (Sigma-Aldrich, St. Louis, MO, USA). Streptozotocin (200 mg/kg) was dissolved in citrate buffer (Sigma) and used within 5 min. Nonfasting blood glucose concentration was measured using a portable glucose analyzer (Beckman Instruments, Fullerton, CA, USA) from samples obtained by tail snipping. Mice with two consecutive nonfasting blood glucose concentration measurements >350 mg/dL were used as recipients.
Islet isolation and preparation
Pancreatic islets were isolated from a healthy nondiabetic mice. The common bile duct of the mouse was cannulated and injected with 5 mL of Collagenase P solution (Roche, Indianapolis, IN, USA) at 0.55 mg/mL in HEPES-buffered Hanks' balanced salt solution. The distended pancreas was excised and digested for 20 min at 37℃. Islets were purified with a discontinuous Ficoll gradient solution. The islets were counted under a dissecting microscope. An algorithm was used to calculate a 150-µm-diameter islet equivalent number (IEQ). One donor yielded 100-200 IEQs. RPMI-1640 (Gibco Laboratories, Grand Island Biological Co., Grand Island, NY, USA) supplemented with 10% fetal bovine serum, glutamine, and antibiotics (penicillin, streptomycin, and amphotericin B; Gibco) was used as the culture medium. Before transplantation, the required number of islets for transplantation was collected manually and prepared for transplantation.
Transplantation of islets to each site
Transplantation was performed about 5 days after the induction of diabetes. Ketamine (100 mg/kg, i.p.) and xylazine (10 mg/kg, i.p.) were used for anaesthesia. The operative time was defined as duration from the first incision to the final skin closure. The operative mortality was defined as the death of a mouse between the first incision until the first week after transplantation. The transplantation methods were as follows. In the kidney, an incision was made on the left flank, the kidney was exposed, and islets were injected via a polyethylene tube (PE-50, Becton Dickinson, Parsippany, NJ, USA) inserted beneath the kidney capsule. In the liver, the bowel was displaced to the left, the portal vein and superior mesenteric vein were identified, and islets were injected into the portal vein in a suspension form in 100 µL of phosphate-buffered saline through a 30 G needle. After islet injection, the lumen of the syringe was rinsed with about 50 µL of portal blood, which was then reinjected to ensure complete injection of the islets. The injected site was compressed for 5 min for hemostasis, and the abdomen was closed carefully. The fluid remaining in the injection syringe was collected and examined under a microscope to identify any residual islets; this examination revealed that <5% of the injected islets remained. For transplantation into the muscle, the hind leg was immobilized, incised to expose the calf muscle, and sharp dissection with microscissors was used to make room for the islet transplantation. Islets were injected via a polyethylene tube, and the opening was ligated with a nonabsorbable suture. In the omentum, an omental pouch was created with some modification of a previous method (12). The greater omentum was identified and spread out before islet transplantation. The islet pellet was placed on the omentum, which was then folded upon itself, and the margin of the omentum was sutured with a nonabsorbable suture.
Graft function analysis
The animals were observed for 3 months after surgery. The nonfasting blood glucose concentration was monitored 3 times a week using a portable glucose analyzer (Beckman Instruments, Fullerton, CA, USA). The graft function was defined as successful when the nonfasting blood glucose concentration was <200 mg/dL and as failure when the nonfasting blood glucose concentration was >200 mg/dL in two consecutive samples. The marginal mass was defined as a subcurable dose of IEQ that cured 50% of the engrafted diabetic mice. The time to reach euglycemia was defined as the number of days before blood glucose concentration lower than 200 mg/dL. The IPGTT was performed each month after transplantation. Briefly, after an overnight fast, 1.5 g/kg body weight of a 20% dextrose solution was injected, and the blood glucose concentration was measured after 0, 2, 5, 10, 20, 40, 60, 90, and 120 min.
Histological examination
Serial sections of the islet-bearing organs or tissues were obtained to evaluate the morphology by staining with hematoxylin-eosin (H&E) and dithizone (Sigma) 45 or 90 days after transplantation. Samples were embedded in OCT 4583 compound (Miles Inc., Elkhart, IN, USA), snap-frozen in liquid nitrogen, and preserved at -70℃ in a deep freezer until sectioned. The pancreas of a normal mouse was used as the positive control for insulin staining. The islets implanted into the omental pouch and kidney subcapsule were obtained by omentectomy and nephrectomy, respectively, and the islets transplanted into the liver were obtained by hepatectomy. Graft-bearing calf muscle excision was used to obtain the islets transplanted into the muscle. Staining with dithizone was used to identify the islets rapidly. The section was then processed for H&E staining.
Statistical analysis
All results are expressed as the mean±standard error of the mean (SEM) for the number of experiments indicated. The data were analyzed using analysis of variance (ANOVA). The Bonferroni correction was applied for multiple comparisons by dividing the P value by the number of comparisons. A P value <5% was considered significant.
RESULTS
Operative feasibility
The operative feasibility was assessed as the operative time and mortality rate (Table 1). Islet transplantation to the kidney subcapsule and muscle required a very small incision, which resulted in the short operation time of 10.2±0.4 min and 11.2±0.4 min, respectively. Manipulation of these sites caused few fatal problems and resulted in low mortality rates of 6.7% and 7.1%, respectively. Transplantation into the liver and omentum took 27.4±1.3 min and 19.8±0.9 min respectively because of opening and closing of the peritoneum. The operative mortality rate was 20.0% in the liver group and 12.5% in the omentum group. The liver group had the highest operative mortality and longest operative time, probably because the procedure involved direct access to the portal vein, which might have caused bleeding that required extra time for hemostasis.
Implantation efficiency
Glycemic control was investigated after decreasing volumes of islets were transplanted into each site. This sequential transplantation was performed in the four transplantation sites. The kidney group showed more consistent glycemic control than the other groups (Fig. 1), and incidental hyperglycemic event after transplantation occurred rarely. In the kidney group, the mean time to reach euglycemia after transplantation was 3.0±1.0 days, which was the shortest of all groups (Table 1). The kidney subcapsule was the most efficient site for islet transplantation in terms of the marginal mass because it required only 100 IEQs, the smallest value for all sites (Fig. 2). The liver and muscle groups had a similar glycemic control pattern, which showed poor glycemic control and took longer time to function than in the other groups. The mean time to reach euglycemia was 15.1±3.3 days in the liver group and 26.6±5.9 days in the muscle group. The marginal mass for both groups was 600 IEQs. Blood glucose concentration was controlled strictly in the omental pouch group, and the time to function (13.9±3.7 days) was shorter than in the liver and muscle groups. The marginal mass was 200 IEQs in the omental pouch group. A prompt return to hyperglycemia after the removal of the islet graft in the kidney subcapsule, muscle, and omental pouch groups demonstrated that the blood glucose concentration was controlled by the islet grafts and not by the residual endogenous islet. We could not remove the islet graft from the liver group because a hepatectomy is not a survival surgery. The correlation between the mean time to reach euglycemia and transplanted isle volume was assessed but was not statistically significant.
Glycemic control efficiency
The glucose tolerance test was performed only in the mice that had been cured of hyperglycemia by successful islet transplantation. Fig. 3 shows the blood glucose concentration after glucose challenge in each group. The area under the curve (AUC) was calculated and the differences in glucose clearance kinetics between groups were analyzed by ANOVA. The omental pouch group showed the most effective glucose clearance, which did not differ significantly from that in the normal control animal. Other sites showed poor glucose clearance kinetics. Muscle showed the most delayed and lowest glucose clearance rate.
Histological findings
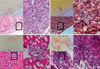
Fig. 4 shows the histological findings of the engrafted islets in each transplantation site stained with dithizone and H&E 3 months after transplantation. The dithizone staining on unfixed cryosectioned tissue revealed insulin-containing islets promptly. Further staining with H&E showed intact and well-preserved islets without surrounding steatosis in the tissue of each transplantation site.
DISCUSSION
Our study demonstrates the characteristics of each islet implantation site, including the kidney subcapsule, liver, omental pouch, and muscle, and that each has advantages in terms of the operative feasibility, implantation efficiency, and glycemic control efficiency. Although many studies have investigated the ideal islet implantation site using various characteristics, none has compared the four sites within the same recipient-donor pair and according to the same parameters. In this respect, our study provides unique data. Using one operator and comparing the four sites, one study allowed us to exclude variables that could influence the experimental results. One advantage of our study is our measurement of implantation efficiency, which allowed us to determine the actual marginal mass or the subcurable dose that can cure diabetes in 50% of recipients for each site. The transplanted islet mass was scaled down by 100 IEQs from the large volume of islets enough to cure diabetes; for example, the mass was 1,500 IEQs in the muscle group and 300 IEQs in the kidney group. The largest islet mass that could no longer control hyperglycemia was defined as the tentative marginal mass. Finally, the marginal mass was identified by increasing the number of transplantation cases with the amount of islets around the tentative marginal mass. This sequential dose-decreasing method differs from that used in previous studies, in which the same amount of islets was transplanted into different sites, and the implantation efficiency was measured only by comparing the success rate (6-8, 11).
An ideal graft recipient site (10, 13, 14) should provide an easy access for transplantation and retrieval, a safe procedure, a trophic effect for maximal islet graft and survival, effective hormone secretion within the physiologic location and immunologic privilege for inducing a donor-specific unresponsiveness in the allograft. It should also reduce molecular incompatibility associated with islet destruction between the donor and recipient when used in the xenograft. The parameters used in our study could provide the right information to evaluate all these factors except for the latter two. However, determining the operative feasibility, implantation efficiency, and glycemic control efficiency in a syngeneic mouse model could provide suitable background data to determine an optimal site in allogeneic and xenogeneic models.
The kidney and liver are the most extensively studied organs as candidates for islet implantation sites. In our study, the kidney gave the best results, with the shortest operative time, lowest operative mortality, smallest marginal mass, shortest time to reach euglycemia, and strictest glucose control. However, the human kidney subcapsule is inelastic and has limited space beneath it that cannot accommodate large amounts of islets, and the implanted islets can deteriorate easily because of exocrine contamination (15). These critical limitations restrict the clinical application of islet transplantation into the kidney subcapsule. One report on human allograft transplantation into a kidney site had poor results (16).
Successful human allo-islet transplantation (1) has made the liver the standard organ of choice for islet transplantation. The intraportal islet transplantation procedure is very simple. Achieving a high drug concentration in the portal vein may increase the chance of tolerance induction with a lower total drug administration volume (17). However, the portal vein infusion procedure causes immediate destruction of large amounts of islets (3), and this phenomenon would be more evident in the xenograft setting because of the molecular incompatibility between species (18). The portal transplantation of islets can induce hepatocellular carcinoma (19). In terms of the physiology, one study reported on the placement of embolized islets within hepatic cords along the distal sinusoid (20). Most of the secreted insulin is released directly into the systemic circulation, so most hepatocytes are not exposed to high insulin concentrations (21), leaving focal, microscopic regions of liver that receive insulin. This may explain why the liver group showed no physiological advantage in the IPGTT study. The large volume of marginal mass and high mortality rate in our study do not support the idea of the liver as an ideal islet transplantation site. It was surprising that implantation to the liver via the portal vein showed shorter function recovery time than expected. For unknown reasons, there have been very few reports on syngeneic mouse islet transplantation into the liver. We speculate that the high mortality rate and delayed recovery of function might have contributed to this. One report with details of individual glucose levels (22) showed a shorter recovery time than we found here, but somewhat delayed implantation.
Muscle is thought to provide easier surgical access (9). This is consistent with our operative feasibility assessment showing a low mortality rate and short operative time. The muscle could provide a safer route for xeno-islet implantation than the portal vein by decreasing the effect of immediate islet destruction, which may be stronger in the xenogeneic setting because of the molecular incompatibility. However, the lower angiogenic potential or vascularity would be a major drawback. This site took more time to function and required a large amount of islets compared with the other sites investigated. Despite these limitations, further study should focus on improving the engraftment by enhancing angiogenesis because the muscle site provides a significant logistical advantage and minimally invasive route.
The omentum has a major disadvantage in that repeated transplantation is not allowed. For the same reason, it cannot be an islet transplantation site in a patient who requires laparotomy for any reason. Furthermore, access and manipulation of the omentum may offer minimal risks of intestinal adhesion and obstruction. However, the omentum offers some advantages. First, its blood supply and drainage resembles the original islet-blood relationship (12). In our study, islets in the omental pouch produced a glycemic AUC that was most similar to control animals in terms of the IPGTT, reflecting a physiologically normal delivery of insulin. It can be argued that intraperitoneal glucose injections could be an advantage in directly stimulating omentally engrafted islets and could give better glycemic control. Considering the very limited surface area of the manipulated omental pouch attached to the stomach wall, the chance for the islet to contact glucose directly during an IPGTT performed at least one month after transplantation would be negligible. Intravenous glucose tolerance testing might confirm this point. Second, it can accommodate a large islet volume (12). This characteristic feature may provide enough space for encapsulated islets or cotransplanted material. Third, the omentum offers better survival (23) of unpurified islets than do other sites. Considering the low purity of isolated human islets, this site may offer a great advantage for allogeneic islet transplantation.
To assess the glycemic control efficiency, we performed an IPGTT each month after transplantation during the observation period and found that the glucose clearance did not change over time. For this reason, for those mice undergoing graft resection before 3 months, the AUC obtained from the first month's IPGTT was used for comparison. Even though we compared the successful groups, these were heterogeneous in terms of islet volume. However, there was no significant difference between the four lowest and four highest volumes of islets among the eight successful recipient mice for each site (data not shown). It is known that once above the threshold, further increase in islet mass is not associated with any increase in glucose clearance (24).
Eventhough we tried to evaluate four implantation sites for pure islets engraftment capacity comparisons for clinical application, it has some limitations. First, this syngeneic mouse model does not allow assessment of immunologic rejection or molecular incompatibility between the donor and recipient. Therefore, the same results would not be expected in allogeneic or xenogeneic islet transplantation models. Second, the results of small animal experiments might not be applicable directly to large animals or humans. Third, islet transplantation via portal vein is usually performed percutaneously by radiologic intervention in clinical setting. This differs from this study method in which laparotomy was inevitable. In this regard, the operative time and mortality of liver transplantation group might have been overestimated. Fourth, six fold higher numbers of islets to cure mice after intraportal transplantation and fifteen days for normalization of blood glucose requires further optimization of transplantation technique.
However, our results imply that the omental pouch could be the optimal site in terms of implantation and glycemic control efficiency, although the results in IPGTT would be overestimated due to the direct contact between the challenged glucose and the implanted islets. On the other hand, muscle could be an attractive site of choice in terms of operative feasibility. If only an engraftment enhancing method is developed, muscle could be an excellent alternative site.
In summary, we evaluated and compared islet transplantation into four sites in terms of the marginal mass, operative feasibility, and glycemic control efficiency. A strategic approach is required for deciding on the best transplantation recipient sites after considering the available donor source and volume of islets. Alternatives can be chosen based on safety or efficacy.




 XML Download
XML Download