

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pleomorphic carcinoma of the lung is defined as a group of poorly differentiated non-small cell carcinoma that contains a component of sarcoma or sarcoma-like elements and shows carcinomatous as well as spindle and/or giant cell components [1]. Pleomorphic component should comprise at least 10% of neoplasm. It's a rare tumor that makes up only 0.1% to 0.4% of all malignant lung tumors, and its clinical prognosis is highly unpredictable [2-4].
Elevated serum beta-human chorionic gonadotropin (βhCG) levels have been reported in 12% of NSCLC patients [5]. When immunohistochemical methods are used, βhCG positivity have been detected in 28% of the resected specimens [5]. Although βhCG production is not seen rarely in NSCLC, clinically significant symptoms, e.g. gynecomastia are uncommon.
Here we describe a 50-yr-old male patient with pulmonary pleomorphic carcinoma producing high levels of βhCG and presenting with gynecomastia.
CASE REPORT
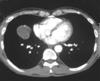
A 50-yr-old man with a history of smoking presented with bilateral gynecomastia and weight loss on December 4, 2008. Physical examination showed bilateral slightly enlarged breasts. Although his serum AFP level was in normal range, his serum βhCG level was found to be elevated (6,500 MIU/mL). Physical examination of the testes and testicular ultrasonography did not detect any mass formation. Chest radiography revealed a right paracardiac opacity. Computed tomography (CT) showed a solitary mass in the right middle lobe (Fig. 1). In PET scan, a solitary hypermetabolic lesion (SUV: 12), 6 cm in size, was identified in the right middle lobe. The brain MRI detected no abnormalities. After excluding the presence of any middle zone tumors and lymph node involvement , excision of right lung lesion was planned.
The pleural cavity was entered through a right thoracotomy at the fifth intercostal space. The mass was explored in right middle lobe. Well-shaped mass located in the right middle lobe was seen; frozen section performed during operation identified malignancy, therefore a decision for right middle lobectomy was made. Major and minor fissures were divided free. Middle lobe arterial branches were explored and freed circumferentially by sharp and gentle blunt dissection and tied with 2-0 silk sutures and divided between ligatures. Middle lobe vein was isolated, ligated and divided between ligatures. Middle lobe bronchus was dissected free and a TA 30 stapler was used to close the bronchus. After the staple line had been placed, a bronchus clamp was placed distal to the staples. Right middle lobectomy and mediastinal lymph node dissection were performed. Operation was finished without complication.
Pathological examination of lobectomy material revealed a peripherally located, 5 cm-in diameter, cavitary tumoral lesion. Microscopically, the tumor consisted mostly of polygonal pleomorphic cells, intermingled with few inflammatory cells (Fig. 2A). There were limited number of carcinoma foci with squamoid differentiation. Some non-cohesive multinuclear giant tumoral cells (giant cell component without syncytiotrophoblast) were seen in a few areas. The diagnosis of pleomorphic carcinoma was made due to cytokeratin immunopositivity in most of the tumor cells. βhCG and PLAP expression was present in approximately 40% of the multinuclear giant and polygonal cells on immunohistology, but the tumor cells were negative for TTF-1 (Fig. 2B, C). There was no tumoral involvement in the mediastinal and hilus lymph nodes.
After surgery, serum βhCG level decreased gradually. At third day after operation, sudden loss of conciousness and respiratory distress occured; urgent cranial CT scan was done. Right cerebellar infarction, closure of fourth ventricules and hydrocephalus were observed. In emergency conditions suboccipital craniotomy, right cerebellar infarctectomy and ventricular drainage were performed, pathology of resected material diagnosed cerebellar subacute infarction. Anticoagulant therapy was started. Tracheostomy and gastrostomy were applied.
Serum βhCG levels increased gradually in time during the patient's follow-up suggesting relapse or metastasis (Fig. 3) and subsequently a positron emission tomography scan was obtained which revealed a 3×4 cm in size, pleura-based lesion with a SUV of 6.2 located in the superior-posterior segment of the right hemithorax and FDG positive enlarged mediastinal lymph nodes. Histopathological verification of transthorasic fine needle aspiration biopsy material was consistent with pleomorphic carcinoma. Therefore chemotherapy was started with the indication of recurrent lung cancer. After two cycles of cisplatin-etoposid based chemotherapy, the levels of serum βhCG decreased dramatically (Fig. 3) and regression in the size of the lesion was observed through CT scan. Four months after the start of chemotherapy, the patient presented with headache and somnolence. Brain MRI showed multiple metastatic lesions with the largest one being 3 cm in diameter and accompanying perilesional edema. Antiedema treatment was started and palliative whole brain radiotherapy was performed. The patient died 2 months later from respiratory failure due to progression of brain metastases and cerebral edema resulting herniation.
DISCUSSION
In the 1999 WHO/International Association for the Study of Lung Cancer Histological Classification of Lung and Pleural Tumors, primary pulmonary choriocarcinoma is described as a miscellaneous tumor [1]. Primary extragonadal choriocarcinoma is very rare and when it occurs, it is usually located in the mid-line structures, mainly the retroperitoneum, mediastinum, or cranial cavity, although other sites have been reported. One of the least common sites is the lung [6]. Large cell carcinoma and pleomorphic carcinoma may occasionally include pleomorphic multi-and/or mononucleated tumor giant cells, which are similar to syncytiotrophoblastic cells and cytotrophoblastic cells of choriocarcinoma. This pathological image is sometimes confusing. In our case's histopathological investigation syncytiotrophoblastic and cytotrophoblastic cells were not seen. Giant cells suggesting choriocarcinoma stained positive for germ cell markers such as βhCG, HPL and PLAP, but were negative for TTF-1; so that tumor was not exactly derived from the lung. In the light of these findings this tumor was diagnosed as pleomorphic carcinoma of the lung with a giant cell component and expressing βhCG.
βhCG is used for detecting and managing gestational trophoblastic diseases, diagnosing quiescent gestational trophoblastic disease, diagnosing placental site trophoblastic tumor, managing testicular germ cell malignancies, and monitoring other human malignancies [7]. βhCG is usually produced in the human placenta. Although βhCG synthesis in NSCLC is well-known, βhCG producing pleomorphic carcinoma is very rare [8, 12]. Thus, to our knowledge this is the third case of pleomorphic carcinoma of the lung producing βhCG in the literature. Another important issue in our case is, elevated serum βhCG levels were associated with clinically significant gynecomastia. Gynecomastia is reported in some gonadal and extragonadal originated cancer types as a paraneoplastic syndrome [9, 10]. But again to our knowledge our case is also the first case with gynecomastia in pleomorphic carcinoma of the lung. As expected, with decreasing levels of βhCG after treatment gynecomastia gradually regressed.
The association between serum βhCG levels and recurrence in patients with lung cancer were previously reported in the literature [5, 11]. In our patient, βhCG levels decreased after surgery, elevated with recurrence, and decreased again with chemotherapy. Hirano et al. had suggested that pleomorphic carcinoma patients with immunohistochemical positivity for βhCG have an elevated risk of local recurrence and metastasis [12]. Although our patient initially presented with a stage IB tumor, recurrence occurred in the postoperative 4th month. Therefore elevated βhCG levels may be associated with aggressive clinical course and increased risk of recurrence in patients with pleomorphic carcinoma expressing βhCG. Furthermore it may have an useful role for evaluation of recurrence and therapy response.
In patients with lung carcinoma, cases about development of cerebral infarct during or after surgical approaches (pneumonectomy or lobectomy) for primary tumor have been reported rarely in the literature. In these cases tumor embolies originating from tumor cells disseminating to systemic circulation through pulmonary vein in the course of surgical procedures are held responsible [13, 14]. Risk factors associated with arterial thromboembolism in patients with lung carcinoma are chemotherapy (especially cisplatin based) [15], targeted therapy (bevacizumab) [16], tumor induced nonbacterial thrombotic endocarditis [17] and disseminated intravascular coagulation [18]. Acute cerebral infarction due to tumor emboly developing after lobectomy for brain metastases was described in a case report [14]. However in our case, there were no tumor cells in histopathological examination of resected cerebral infarct material. Furthermore any of the risk factors related with arterial thromboembolism were absent in our case. In the light of these findings, we hypothesize that cerebral thromboembolism may have occurred due to hypercoagulability state associated with the primary tumor.
In conclusion, pleomorphic carcinoma is one of the rare tumors of the lung with clinically unpredictable course. Our patient is the first case of pleomorphic carcinoma of the lung presenting with gynecomastia reported in the literature. Elevated βhCG levels may be associated with early recurrence and poor prognosis in patients with pulmonary pleomorphic carcinoma.


 XML Download
XML Download