

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Incontinentia pigmenti (IP; MIM 308300) is a rare X-linked dominant disorder characterized by abnormal skin pigmentation, retinal detachment and central nervous system defects (1, 2). This syndrome is typically lethal in male but female patients survive as cells expressing the mutant X-chromosome are selectively inactivated. Such negative selection usually results in IP female patients showing an extremely skewed X-chromosome inactivation (XCI) pattern as compared to approximately 10% in a healthy population (3, 4).
The pathogenesis of IP is associated with mutations in the nuclear factor κB essential modulator (NEMO), also known as IKBKG (IKK-gamma gene). The NEMO encodes a regulatory component of the IkB kinase complex that is required for the activation of the transcription factor NF-κB and is fundamental for cell development, survival and function (5). The gene, located on chromosome Xq28, is composed of 10 exons with three alternative noncoding exons. A highly homologous pseudogene, so-called 'ΔNEMO', also exists within a 35.5 kb duplicated fragment opposite to NEMO, and contain NEMO exons 3 to 10. A large deletion of NEMO exons 4 to 10 is found in approximately 80% of IP patients, whereas other mutations such as small nucleotide substitution, deletion and insertion account for a small proportion of patients (5, 6). The deletion alters sequence after nucleotide 399 (from ATG) in the NEMO mRNA and leads to a truncated protein containing the first 133 N-terminal amino acids (1). Although many IP patients have been described in the literature (7), there are no genetically confirmed patients in Korea. In this study, we performed a genetic analysis for Korean patients clinically diagnosed with IP and found the common genomic rearrangement that involved the deletion of exons 4 to 10 in NEMO.
CASE REPORT
Clinical findings
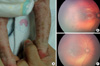
Four unrelated female patients with clinical features of IP were evaluated. All patients were diagnosed shortly after birth as presenting with progressive erythema, vesicular rash and linear hyperpigmentation on the limbs and trunk. Patient 1 was a 15-month-old girl who presented with a linear vesicular eruption on the extremities since birth. On examination, the patient had vesicles and crusted lesions on the extremities, accompanied by swirled hyperpigmentation on the arm, foot and abdomen (Fig. 1A). A fundus examination revealed retinal hemorrhage and macular hypopigmentation in both eyes (Fig. 1B, C). There was no family history of skin disease. Patient 2 was a 19-month-old girl, with a recurrent linear vesicular eruption on the extremities since birth. The patient had no family history of skin disease. Hematological analysis on admission showed marked eosinophilia (32%) with leukocytosis (23,000/µL). A fundus examination revealed retinal hemorrhage in the left eye and developmental milestones were delayed. The mother of the patient had multiple miscarriages. Patient 3 was a 21-month-old girl who also presented with characteristic features of IP including hyperpigmented skin lesions, hypodontia and a family history of skin disease. Slightly delayed developmental milestones were also observed. The mother was noted to have similar skin manifestations and the maternal grandmother had two episodes of miscarriage. Patient 4 was a 27-yr-old female who had one previous miscarriage at 13 weeks gestation. She was diagnosed with IP based on skin manifestations and a family history of skin disease during early childhood (her mother and older sister had similar skin manifestation). A physical examination was unremarkable other than skin manifestation.
A recurrent mutation in NEMO
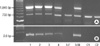
After obtaining written informed consent, PCR-based analyses were performed in the four patients, the parents of Patient 3 and two healthy control subjects in February, 2008. This study was approved by the Samsung Medical Center Institutional Review Board. Multiplex PCR was performed to identify the common deletion as either NEMO or ΔNEMO by using two forward primers (Int3s and Rep3s) and one single reverse primer (L2Rev), described by Steffann et al. (Fig. 2) (8). A 1045-bp sized product was expected for the deletion involving exons 4 to 10 of either the NEMO or ΔNEMO (Int3s and L2Rev), whereas a 733-bp product was expected in all tested participants as an internal amplification control (Rep3s and L2Rev). Confirmatory long-range PCR was also performed to detect the specific genetic rearrangement of the NEMO, described by Bardaro et al. (9). A 2.6-kb product was expected for the pathological NEMO deletion with a forward primer (In2) and a reverse primer (JF3R). In a comparative PCR assay performed with JF3R and a ΔNEMO-specific reverse primer (Rev-2), a 2.5-kb product was expected for the ΔNEMO deletion.
For the multiplex PCR analysis, all tested individuals showed the 733-bp product, whereas only the four female patients and the mother of Patient 3 showed the 1045-bp product (Fig. 3A). For the long-range PCR analysis, the expected 2.6-kb product was seen in only the four patients and the mother of Patient 3 (Fig. 3B). Also, in a comparative PCR assay performed with JF3R and a ΔNEMO-specific reverse primer (Rev-2), the expected 2.5-kb product was not detected in all tested individuals. These results indicate that the deletion was in the NEMO and not in the ΔNEMO.
X-inactivation analysis
The XCI pattern was determined by PCR analysis of a polymorphic CAG repeat in the HUMARA (10). After digestion with the methylation sensitive enzyme HpaII, a PCR product is obtained only from the inactive X-chromosome. The PCR products were analyzed by GeneScan Software. XCI was calculated as the ratio between the intensities of the PCR products of the two alleles with the smallest allele given first. The presence of skewed XCI was considered if the ratio was ≥65:35, and considered extremely skewed if the ratio was ≥80:20 (11). The heterozygous alleles of the X-chromosomes in each non-digested sample were shown with a CAG repeat polymorphism (Fig. 4). After DNA was digested with HpaII, Patient 1, Patient 4 and the mother of Patient 3 showed only one of the heterozygous alleles, indicating that these had a highly skewed XCI. Patient 2 and Patient 3 showed one distinct peak and one faint peak. These results indicate that all affected individuals had a skewed XCI, although the degree of skewing was different.
DISCUSSION
Bardaro et al. have reported the use of a long-range PCR method that discriminates between rearrangement in the NEMO and ΔNEMO, thus enabling molecular diagnosis for IP (9). However, the absence of an internal control for PCR precludes discrimination between PCR failure in rearranged individuals and the absence of NEMO or ΔNEMO rearrangement, giving false-negative results. Subsequently, Steffann et al. proposed the use of a multiplex PCR method to overcome these limitations (8).
In this study, all affected individuals showed an identical genomic rearrangement involving a deletion of exons 4 to 10 of the NEMO. It has been reported that in Western countries, an identical genomic deletion accounts for 80% of the identified mutations in the NEMO (5). As the same mutation was found in Korean and Japanese IP patients (12, 13), the deletion may be the most common mutational hot spot irrespective of the ethnic background, although the number of the patients was limited.
In this study, the method proposed by Bardaro et al. has been demonstrated to be reproducible; however, we experienced difficulty to identify optimal PCR conditions for DNA amplification. In addition, long-range PCR is a time-intensive and labor-intensive method as compared with multiplex PCR. Therefore, we suggest that the multiplex PCR proposed by Steffann et al. may be useful for screening the existence of the NEMO rearrangement for clinically suspicious IP patients, and the use of long-range PCR proposed by Bardaro et al. should be considered as a confirmatory diagnostic tool for patients with positive findings with screening multiplex PCR testing.
All the four patients showed the classical cutaneous signs of IP and the observed clinical manifestation spectrum was similar to that previous Korean IP study report by Kim et al. (14). For the XCI analysis, all affected individuals showed a skewed XCI pattern. Two patients (Patients 1 and 4) and the mother of Patient 3 showed an extremely skewed XCI and two patients (Patients 2 and 3) showed mild skewing of XCI. The XCI phenotype might be related to the disease phenotype, since Patients 2 and 3 showed relatively severe clinical manifestations such as developmental delay, hypodontia and retinopathy, although all affected individuals had the same mutation. Martinez-Pomar et al. (15) described an IP patient with severe clinical manifestations in the first 30 months of life. At that time, the patient showed a random XCI pattern. At the age of 42 months, however, all clinical signs disappeared, and a completely skewed XCI pattern was observed. Therefore, XCI could modify the clinical phenotype of IP, but has limitations to explain all of the phenotypic manifestations of IP.
This is the first report of genetically confirmed IP patients in Korea. The patients showed a common genomic rearrangement involving the deletion of exons 4 to 10 in NEMO and the mutation spectrum was similar to that previously reported. Although only a small number of patients was investigated, this study indicates that the genetic analysis of the NEMO may be helpful for rapid confirmation of IP diagnosis, prenatal diagnosis and carrier detection.


 XML Download
XML Download