

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cervical cancer is the second most common cancer affecting women worldwide and also an important complication of genital HPV infection; approximately 500,000 women are diagnosed with this type of cancer, and around 270,000 women die due to it each year (1). In Korea, cervical cancer is the 5th most common female cancer with 4,949 reported cases in 2002 (2) and the 5th leading cause of death among Korean women (3) with new cases of cervical cancer accounting for 9.8% of female cancers (4). The overall age-standardized incidence rate of cervical cancer from 1999-2002 was 15.1 per 100,000 women (5).
Persistent infection with genital HPV types 16 and 18 is associated with a greatly increased risk for subsequent development of invasive cervical cancer (ICC) (6, 7). Data from a meta-analysis study on the overall and type-specific HPV prevalence in 13,842 Korean women showed that in ICC, HPV types 16 and 18 accounted for 65.1% of cases (8). HPV-16 and 18, and HPV-45 are the most commonly detected HPV types in women with cervical adenocarcinoma and squamous cell carcinoma (SCC) (9). It is suggested that greater than 50% of all sexually active women will be exposed to at least one genital HPV at some point in their life (10). In a meta-analysis of a systematic literature review, young women aged below 25 yr were found to have the highest prevalence of HPV infection (11), whereas persistent HPV infections became more prominent with increasing age (12). HPV infections are seen to be the highest in adolescent populations (13) and most are acquired soon after initiation of sexual activity. Considering the natural history of HPV infection, the optimal target age for immunization are pre-adolescent girls in order to provide them with protection before sexual debut.
The HPV-16/18 AS04-adjuvanted vaccine is now licensed in over 90 countries worldwide and has been shown to be highly efficacious, immunogenic and generally well-tolerated in previous global studies (14, 15). In addition, the vaccine was also highly efficacious in the prevention of incident and persistent HPV-16/18 infections and in the maintenance of cross-protection against incident infections caused by HPV-31 and HPV-45 for at least 6.4 yr of follow-up (16). Vaccine-induced immune responses in young female adolescents were approximately two-fold higher than those elicited in women aged 15-25 yr (17). Though there are several studies on the HPV-16/18 AS04-adjuvanted vaccine worldwide (14-17), there has been previously no data of this vaccine in the Korean population.
Thus, the present phase III study was performed to evaluate the immunogenicity and safety of the HPV-16/18 AS04-adjuvanted vaccine in Korean girls aged 10-14 yr.
MATERIALS AND METHODS
Study population
A total of 321 healthy pre-adolescents and adolescents females 10-14 yr were enrolled in the study (Clinical trial Number - NCT00290277) from eight centers in Korea between November 2005 and August 2006.
The study protocol, amendments and consent forms were approved by the Institutional Review Board (KCMC05MT092, 05-40, H-0509-509-157, 2005-0258-12, 05-36, 2005-09-013-034, 2007-27, 2005-269) of each study center. The study was conducted in accordance with Good Clinical Practice and all applicable local regulatory requirements and the Declaration of Helsinki. Written informed assent was obtained from each subject, and written informed consent was obtained from each subject's parent/legally acceptable representative before entry into the study.
Subjects were required to be healthy, not taking any other investigational products or immune-modifying drugs, not pregnant or planning to become pregnant, or breastfeeding during the study. Subjects with child bearing potential were required either to be taking effective contraception or abstinent from sexual relations. Pregnancy tests were conducted prior to each vaccination. Subjects were not to have received previous vaccination with a HPV vaccine.
Study objectives
Primary objective: To assess the immunogenicity of the HPV-16/18 AS04-adjuvanted vaccine one month after the third vaccine dose.
Secondary objectives: To evaluate vaccine reactogenicity and safety for 30 days after each vaccine dose and throughout the study period.
Study vaccines and study design
The study vaccine (Cervarix™, GlaxoSmithKline Biologicals, Rixensart, Belgium), was an HPV-16/18 L1 (L1 - structural protein of HPV) Virus Like Particle (VLP) vaccine that contained HPV-16 L1 protein (20 µg), HPV-18 L1 protein (20 µg). The vaccine was adjuvanted with AS04 (50 µg of 3-O-desacyl-4'-monophosphoryl lipid A [MPL] and aluminum, Al[OH]3 500 µg) (17, 18).
The control used in this study was hepatitis A virus vaccine (HAV-Havrix™, GlaxoSmithKline Biologicals, Rixensart, Belgium) containing 360 enzyme-linked immunosorbent assay (ELISA) units - EU of inactivated hepatitis A viral antigen and 250 µg of aluminum (Al[OH]3). This vaccine was used rather than an aluminum placebo to provide a benefit to participants.
Participants were randomly allocated to two groups in a 1:1 ratio using an internet-based randomization system, to receive either HPV-16/18 or HAV vaccine. Vaccines were supplied in individual 0.5 mL pre-filled syringes and administered into the deltoid muscle according to a 0, 1, 6 month schedule. Due to differences in the visual appearance of the HPV-16/18 L1 VLP AS04 vaccine and the control vaccine, the syringes were prepared and administered by qualified medical personnel not otherwise involved in study conduct or in the assessment of symptoms, so treatment allocation remained blinded.
During the initial stages of the trial, some vaccine doses were suspected to have been accidentally exposed to freezing temperatures during vaccine shipment to trial sites and were injected to some subjects (HPV-16/18 group, 18; control group, 17) as their first dose. The extent of a possible impact of vaccination with these vaccines on the immunogenicity study endpoints was evaluated and statistical analyses revealed no impact on the validity of results.
Serological evaluation
Blood samples were collected from subjects at baseline (before vaccination) and at Month 7 (one month after the third vaccine dose) to evaluate immunogenicity. Antibodies against HPV-16 and HPV-18 were evaluated in subjects from both groups using a type-specific ELISA as reported elsewhere (18). HAV-specific antibodies were evaluated in subjects from both groups using a commercially available ELISA assay (Enzygnost®, Behring Diagnostics, Malburg, Germany).
Safety evaluation
In the first 30-min post-vaccination period, subjects were observed for any adverse events (AEs) following which they were given diary cards to record observations up to the following visit. These diary cards were designed to record information on specific solicited local AEs (injection site pain, redness and swelling), systemic AEs (fever, headache, fatigue, gastrointestinal symptoms, arthralgia, myalgia, rash and urticaria) and any other unsolicited AEs. Solicited AEs were recorded for 7 days (days 0-6) after each vaccination. The intensity of all solicited AEs was graded on a 3-point scale (Table 1). Urticaria or rash that appeared within 30 min of each vaccine dose was also documented by the investigator. Unsolicited signs and symptoms were reported within 30 days (days 0-29) after each dose. Any changes in hematologic and biochemistry values were assessed in blood samples taken from subjects at baseline and at Month 7. Serious adverse events (SAEs), pregnancies, medically significant conditions and new onset of chronic diseases were also collected throughout the study. Medically significant conditions were defined as conditions that prompted emergency room or physician visits that were not related to common diseases or routine visits for physical examination or vaccination, or SAEs that were not related to common diseases, occurring during the entire study period.
Statistical analysis
Statistical analyses were performed using Statistical Analysis System (SAS) 8.2 (SAS Institute, Cary, NC, USA) and Proc StatXact-5 (Cytel Inc, Cambridge, MA, USA) and all sample size calculations were performed using nQuery 4.0.
The sample size was calculated to demonstrate with at least 90% power that seroconversion rates for each vaccine antigen after the third dose was not less than 90%.
The primary immunogenicity analyses were done on the according-to-protocol (ATP) cohort for immunogenicity, including all subjects meeting eligibility criteria, complying with the procedures defined in the protocol, and for whom assay results were available for antibodies against at least one study vaccine antigen component after vaccination.
Immunogenicity prior to the first vaccination and at post-dose 3 was evaluated for each vaccine antigen. Geometric mean antibody titers (GMTs), seropositivity and seroconversion rates with their 95% confidence intervals (CIs) were calculated.
The primary analysis for reactogenicity and safety was based on the total vaccinated cohort and included all vaccinated subjects, with at least one vaccine administration documented for the analysis of safety and with immunogenicity data available for the analysis of immunogenicity.
The two-sided standardized asymptotic 95% CI for the difference in SAE rates was computed. The comparison was done by subject, considering all SAEs at the same level and then considering individual SAEs.
Incidence rates of solicited AEs (7-day follow-up period) and unsolicited symptoms (30-day follow-up period) were tabulated with exact 95% CIs over all vaccine doses and for each treatment group.
Separate immunogenicity and safety analyses were performed for subjects who had received as their first dose a vaccine which may have been temperature-deviated.
RESULTS
Study compliance was high, with ≥98.8% of subjects in the HPV-16/18 group and all subjects in the control group receiving all three vaccine doses.
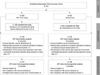
Of the 321 subjects enrolled and vaccinated (HPV-16/18 group, 160; control group, 161), 319 (158 in the HPV-16/18 group and 161 in the control group) completed the study. The parents of two subjects (both in the HPV-16/18 group) withdrew their consent; none of which were due to AEs. The mean age of subjects in the total vaccinated cohort at the time of the first dose was 11.9 yr (standard deviation [SD]±1.41). Both groups and analysis cohorts were well balanced with respect to baseline demographic characteristics, such as age and race.
A total of 248 subjects met the eligibility criteria for the ATP immunogenicity analysis (Fig. 1).
Immunogenicity (ATP cohort)
Immunogenicity analyses were stratified by serology status at baseline and seroconversion rate for each HPV antigen was calculated in subjects who were seronegative for the HPV-16 or HPV-18 antigen. The majority of subjects (up to 89.9% in each group) were seronegative for both HPV-16 and HPV-18 antigens. About 10% of subjects in the HPV-16/18 group were seropositive at baseline for either HPV-16 or HPV-18 antigens.
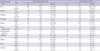
In the HPV-16/18 group, seroconversion rates for HPV-16 and HPV-18 antigens in initially seronegative girls were 100% at Month 7. The geometric mean titer (GMT) was 19619.8 EU/mL (95% CI: 17188.6-22394.8) for HPV-16, and 9894.5 EU/mL (95% CI: 8674.1-11286.6) for HPV-18. All initially seropositive girls remained seropositive for both antigens at Month 7 with markedly higher GMTs than those observed before vaccination and were similar to GMTs in initially seronegative girls (Table 2).
In the control group, the seroconversion rate for anti-HAV antibody at Month 7 was 100% in initially seronegative girls. Anti-HAV GMT was also high at Month 7. Immunogenicity analyses on the total vaccinated cohort were consistent with the results of the ATP cohort analyses. Immunogenicity analyses conducted in girls who had received a vaccine which may have been temperature-deviated did not show any impact.
Reactogenicity and safety (Total vaccinated cohort)
Compliance in returning diary cards was high (>99% in the two groups). Subjects from the HPV-16/18 group reported more injection site symptoms (pain, redness and swelling) than the control group. The most commonly reported symptom was injection site pain (Table 2). Local symptoms tended to be transient, lasting no longer than 4-5 days. These group differences in injection site reactions however had no impact on compliance with completion of the vaccination course. The frequency of local symptoms with grade 3 intensity following vaccine doses remained low in the HPV-16/18 group (up to 2.3% overall). None of the subjects in the control group reported any local symptoms of grade 3 intensity. No urticaria or rash was reported in the 30-min post-vaccination observation period. The incidence of systemic reactions, was generally comparable between groups, with the exception of myalgia reported more frequently in the HPV-16/18 group. Overall, grade 3 systemic reactions were reported infrequently in both groups, with no reports of grade 3 myalgia in either group. Neither group showed an increase in reactogenicity for local and general AEs with increasing number of doses.
Unsolicited AEs occurred with similar frequencies in both groups. The most frequently reported unsolicited AEs in both groups were infections such as upper respiratory tract infections, nasopharyngitis and rhinitis, and dizziness. A minority of the unsolicited symptoms in both groups (2.1% of doses in the HPV-16/18 group and 0.4% of doses in the control group) were considered by the reporting investigator as possibly vaccine related.
The onset of chronic diseases that were identified during the study were contact dermatitis and urticaria (each symptom reported by two subjects in the HPV-16/18 group) and atopic dermatitis (one subject in the HPV-16/18 group and two subjects in the control group).
One vaccine recipient in the control group reported a SAE (gastroenteritis) after the second dose, that required hospitalization. This SAE was judged as not being vaccine-related, resolved without sequelae and the subject completed the vaccination course. No pregnancies were reported. The occurrence of medically significant conditions reported during the study period was similar in both groups (HPV-16/18 group: 6.9%; control group: 6.2%). No clinically significant modification of hematological or biochemical parameters was observed in girls when these parameters were assessed at study entry and at Month 7.
Reactogenicity and safety results in girls who had received as their first vaccination a vaccine that may have been temperature-deviated, were similar to that of girls in the per-protocol cohort.
DISCUSSION
This study was conducted in a cohort of pre-pubertal girls and young adolescents in Korea. An online survey of behavioral health factors in 80,000 Korean adolescents aged 12-17 yr suggests that sexual onset occurs at a relatively early age of 14 yr (19) as compared to that reported in previous data (20). Young age at onset of sexual activity was identified as one of the significant risk factors for HPV infection in two HPV prevalence surveys conducted in Busan, Korea (20, 21). Due to the lifestyle and sexual behavior of Korean women, the prevalence of HPV infection is increasing, and cervical cancer remains a major public health concern in Korean women. Hence, vaccination against the most prevalent HPV types 16 and 18 has the potential to significantly reduce HPV infection and its consequences in Korea (22).
In our study, all initially seronegative subjects seroconverted to both antigens. At Month 7, GMTs were over 400-fold higher than natural infection titers for both antigens (14). Initially seropositive subjects remained seropositive and elicited a marked increase in GMTs from those seen before vaccination, which indicates that prior exposure to natural HPV infection does not affect the immune response generated by the HPV-16/18 AS04-adjuvanted vaccine. The high GMT levels generated in initially seropositive women are important as there is no clear evidence that natural immune response is reliably protective against reinfection.
The magnitude of antibody titers or GMTs achieved in the current study cohort is in line with another study that evaluated the vaccine in European adolescent girls aged 10-14 yr (17). GMTs elicited in this young age group were twice as high compared to those in women aged 15-25 yr at Month 7. The vaccine has been shown to induce high and sustained anti-HPV-16 and anti-HPV-18 antibody levels and shown to be efficacious against CIN2+ and persistent infections associated with HPV-16/18 up to 6.4 yr after first vaccination in women aged 15-25 yr (16). The final event-driven analysis of a large multinational Phase III trial in women aged 15-25 yr also showed that the HPV-16/18 AS04-adjuvanted vaccine was highly efficacious against CIN2+ lesions associated with HPV-16 and HPV-18 as well as those associated with non-vaccine oncogenic types HPV-31, HPV-33 and HPV-45 (23).
Transudation of high vaccine-induced serum IgG antibodies into cervical secretions is likely to be an important mechanism of protection against cervical HPV infection (24, 25). Apart from the HPV-16/18 AS04-adjuvanted vaccine inducing a robust and persistent immune response in the serum, high levels of antibodies were detected in cervicovaginal secretions (15, 26) and could therefore play a prominent role in local immunity to bind to HPV virus particles (25). Applying the antibody transudation theory, it can be speculated that the higher the systemic immune response elicited by a parenterally administered vaccine, the higher the level of transudated antibodies at the site of infection and as consequence, the better the expected protection and the longer protective duration. This assumption can be extended to the high levels of IgG responses elicited by vaccination in the target age group (10-14 yr) in our study. With the established efficacy in women aged 15-25 yr, it can be extrapolated that the protection in young adolescents will last for at least as long as the sustained efficacy observed in previously published results (16, 27, 28). An advantage of the HPV-16/18 vaccine used in the study was the unique AS04 adjuvant in its formulation. In a previous study, the immune response induced by this AS04 adjuvant formulation was observed as being higher to that induced by the same antigens adjuvanted with aluminum alone (18).
In our study, the safety data in young Korean adolescents showed that the HPV-16/18 AS04-adjuvanted vaccine was generally well tolerated (good compliance with the 3-dose vaccination schedule) and had an acceptable safety profile. This is in line with the results of a pooled safety analysis from 11 Phase II/III trials with the HPV-16/18 AS04-adjuvanted vaccine which showed a favorable safety profile in women of all ages (29). The benefit of prophylactic HPV vaccination in these young girls is underscored, as vaccination in this age group generates a robust immune response exceeding that seen in older women. A strong immune response is of particular importance for young adolescents to translate into sustained protection (17) so they are still protected during their peak exposure to natural infection (30).
The younger age of sexual debut among Korean adolescents and girls has resulted in an increased occurrence of HPV infection in this population (19-21). Therefore, prevention at the earliest stage is of prime importance. WHO recommends vaccination of young women prior to their sexual debut and the inclusion of routine HPV vaccination in a country's national immunization program.
In conclusion, this study evaluated the HPV-16/18 AS04-adjuvanted vaccine for the first time in Korean girls aged 10-14 yr, and confirmed that it is highly immunogenic and well tolerated in this population. With cervical cancer posing such a huge physical, psychological, social and financial burden on women in Korea, prophylactic HPV vaccination could be integrated into the existent vaccination programs for adolescents to help reduce the high disease burden of cervical cancer.

 XML Download
XML Download