

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The falciform ligament extends from the umbilicus upward to the diaphragm, and laterally to form the hepatic coronary ligaments. It represents a potential space, and a few cases of falciform ligament abscess secondary to infectious diseases of the liver and gallbladder have been reported in adults. It is often misdiagnosed as a simple abdominal wall abscess due to the location of the abscess and treated non-operatively, which is usually unsuccessful. Here we report a case of falciform ligament abscess after omphalitis in a child.
CASE REPORT
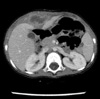
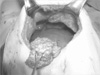
A 2-yr-old male presented with a fever and right upper quadrant abdominal pain. The patient underwent surgery for type three ileal atresia during the newborn period, and had a history of omphalitis two months prior to presentation. On examination the body temperature was 38.6℃ and the umbilicus was normal. There was a firm tender mass palpated in the right upper quadrant of the abdomen. The laboratory test results showed a leukocytosis of 18,290/µL with a shift to the left. The abdominal ultrasound and computed tomography (CT) revealed a 3.4×3.4 cm abscess located at the right paramedian abdominal wall extending to the anterior surface of the liver (Fig. 1). The patient was managed with percutaneous drainage and intravenous antibiotics. The microbiology examination of the abscess identified Methicillin-resistant Staphylococcus aureus (MRSA). Shortly after drain removal, the fever and abscess emerged again and two weeks of intravenous vancomycin and aspiration of the abscess were performed two more times. However, after normalization of the clinical parameters, a follow-up CT revealed a 3.3×2.4 cm residual abscess at the same location. At laparotomy, the abscess was found to originate from the falciform ligament; the abdominal wall was clear (Fig. 2). The falciform ligament was completely excised, and the post-operative course was uneventful. Pathological examination revealed a fibrosis of the ligament with abscess formation. A follow-up ultrasound 2 weeks after the operation showed complete resolution of the abscess. Now it is 4 months after the operation and he is well and healthy.
DISCUSSION
A soft tissue mass beneath the abdominal wall continuous with a thickened round ligament is a diagnostic feature of a falciform ligament abscess by ultrasound or CT scanning (1). However, because of its rarity and obscure location, a definite radiological diagnosis of a falciform ligament abscess is difficult. Infections can extend from the liver, gallbladder (2, 3) and umbilicus (4). An infection of a cystic lesion of the falciform ligament has been reported as a cause of a falciform ligament abscess (5). As shown in this case, it is important to suspect a falciform ligament abscess in a patient with a right upper quadrant abscess and a prior history of abdominal infections.
Lipinski et al. (4) reported two cases of a falciform ligament abscess secondary to an omphalitis; contiguous spread of the infection via the round ligament was thought to be the etiology. In the present case, however, the round ligament was divided due to the previous operation for ileal atresia, because the supraumbilical transverse, round ligament-cutting incision was used to provide more wide operative field. The superficial veins of the abdominal wall form a network that radiates out from the umbilicus, and a few small veins named paraumbilical veins connect the network to the portal vein forming a portal-systemic venous anastomosis (6). This venous network might explain the extension mechanism of the omphalitis into falciform ligament abscess in the absence of a round ligament. Moreover, the paucity of the vascular network inside the ligamentous structure might have impaired the venous outflow from the ligament and the MRSA could be colonized easily within the falciform ligament to form an abscess. Although the round ligament was manipulated during the operation at the neonatal period, the long time interval between the ileal atresia operation and falciform ligament abscess would preclude the possibility of the abscess as a post-operative complication.
MRSA has been reported to be the most frequent causative agent of omphalitis in children (7). The identification of MRSA, which is consistent with the previously isolated microorganisms from the omphalitis, also supports the speculation that the abscess originated from the omphalitis. Delivery at home, low birth weight, use of umbilical catheters, and septic delivery have been known to be risk factors of the omphalitis (8), but the causes of the omphalitis reported here are uncertain. As the omphalitis was cured before the symptoms of the falciform ligament abscess became apparent and there had been no abdominal complaints before the onset of the omphalitis, we speculate that the omphalitis must have preceded the falciform ligament abscess.
Many readily accessible abscesses are treated successfully with percutaneous drainage and the antibiotics. However, in this patient drainage and antibiotics did not completely treat the abscess. This might be also explained by the paucity of the vascular network that hindered exposure to the circulation and therefore the antibiotics. Previous authors reported successful treatment of the falciform ligament abscess after excision of the ligament (4, 9, 10). Therefore, when a falciform ligament abscess is suspected, surgical excision rather than percutaneous drainage should be considered for the initial treatment.
We treated a patient with a falciform ligament abscess secondary to a prior omphalitis. The patient was successfully treated with falciform ligament excision. A strong index of suspicion is necessary for early diagnosis and treatment of similar cases.
 XML Download
XML Download