

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
An objective evaluation is essential for evaluating a disability because the rights of the disabled must be protected. However, it is often difficult to evaluate a disability objectively because the guidelines for disability evaluations have been established quantitatively from the abstract concept that does not exist. The evaluation methods commonly used in this country are the permanent guideline of the American Medical Association (AMA) (1) and the table of McBride (2). The table of McBride is a method that evaluates the loss of labor ability, but the AMA only evaluates the disability. Different or similar guidelines are adjusted according to some of the laws in this country (3). A disability of upper extremity is evaluated by a board of orthopedics, neurosurgery, cosmetic surgery, rehabilitation and industry (Herein defined as 'board'). The departments of orthopedics and rehabilitation have the guideline themselves (4). However, there is some difference in the evaluation of the disability rate between the AMA, McBride and related associations because the disability rate of an amputation, which is a parameter of the disability rate of the upper extremity function, the direction and range of motion that admits the disability, and guidelines for the methods of summing a duplicate disability, are different. There are several reports that have dealt with this in Korea. The aim of this study was to develop the guidelines for evaluating an upper extremity disability based on participation of associated boards as a part of the development of guidelines for evaluating disabilities in the Korean Academy of Medical Sciences.
MATERIALS AND METHODS
In this study, disabilities of the upper extremity were evaluated in the following order: 1) amputation, 2) joint contracture, 3) diseases of the upper extremity, 4) weakness, 5) sensory loss of finger tips, and 6) vascular and lymphatic disease. The order of 1) to 6) is the order of major disability and there is no need to evaluate a lower order disability when there is a higher order disability in the same joint or part of the upper extremity. When there are special contributions from multiple disabilities, the disability of the upper extremity can be either added or substituted so the maximal rate of disability in each joint. Regarding the method of summing, the summed rate (%) of a disability is calculated by the formula, (A+(100-A)×B/100), if the rate of each disability is A (%) and B (%). The maximal rate of a disability in each joint is defined as the maximal rate of a disability when the shoulder, elbow, and wrist joint are completely contractured. The disability rate of the hand was determined by the disability rate of an amputation. An upper extremity disability should be evaluated after treatment is completed and full adaptation is achieved when further functional changes are not expected. The dominance of the right or left hand before a disability occurs should not be considered with a higher rate of disability.
The principle for evaluating each portion is follows. First, the disability rate of an amputation means the maximal function of each joint. Both rates are added if both upper extremities are amputated. Second, the disability of joint contracture is measured from the described table according to the starting and end points of joint motion and it is based on the active range of motion. The active and passive range of motion is different when there is a substantial cause, such as a nerve injury, and an evaluation of the cause is also added. The passive range of motion must be used to examine the disability rate if the active range of motion is much lower than passive motion and there is no definite substantial cause. For example, a decrease in the active range of motion caused by pain must not be considered as a contracture of the joint. Third, the disabilities according to each disease are 1) arthroplasty, 2) instability, 3) dislocation, and 4) deformity, which must be evaluated according to the guidelines for an evaluation of the disability of each disease. This is estimated as a disability from each disease if the contracture is concluded to be less severe than the disability of each disease. For example, in case of shoulder arthroplasty, it is possible to adjust the disability rate of arthroplasty by 18% if the disability rate of the contracture is <14%. Fourth, the disability rate is estimated as a disability of muscle power if the disease exists in the joint but it is not included in the amputation, contracture, and disability according to each disease. For example, there are cases when the muscle power is decreased after a rotator cuff surgery or the hand joint is not well used after a fracture because of arthritis. This corresponds to grades 3, 4 among a manual power examination of 5 grades. A substantial cause, such as a nerve injury, must be surveyed and the radiologic findings or surgical opinion are needed to determine if the disease of the each joint should be given if the grade is below grade 3. Fifth, a disability of hand sensation can be evaluated and added to the disability of the upper extremity because it influences the meticulous upper extremity function. The contribution of each disease to the motion of the upper and lower extremity, sensory nerve injury or disability must be evaluated because the disability of sensation means a functional deficit of the digital nerve below the wrist. Sixth, the disability of a vessel can be evaluated according to the symptoms and examination results, and the functional deficit due to the lymph edema can also be evaluated as a disability of the vessel. It is impossible to combine with other disabilities, and it is estimated as a disability of a vessel if the amputation is concluded to be less severe than the disability of the vessel.
Guidelines for evaluating an upper extremity disability can be formed using the background of the above mentioned principles. An evaluation of a disability of the upper extremity must be estimated objectively. Conflict can occur if the process is easy and a self estimation is possible because the details are open. Therefore, the examination must be performed by an appropriately trained doctor. Rare diagnostic tools must be avoided, and an easy method that can be carried out in the out patient clinic of a general hospital must be used. However, a diagnostic tool by radiation or nuclear medicine is used in the case of a disability according to each disease. An upper extremity disability should be evaluated after the symptoms are fixed and full adaptation is achieved, and a re-evaluation must be performed 2 or 3 yr later if further functional changes are expected.
RESULTS
The evaluation method for each portion is as follows.
The disability of an amputation
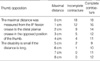
The disability of the upper limb is accepted to be 100% in terms of shoulder disarticulation if the function of the unilateral upper limb is 100%. An amputation at the scapulothoracic level should be accepted for a 110% disability rate of the upper limb because it can increase the functional disability above the function of the upper limb. The disability rate of an amputation depends on the position and residual length of the amputation. The disability rate of a humeral amputation is accepted to be 100% if the amputation is performed above the deltoid insertion because the residual length is short. However, the disability rate is 95% if the amputation is performed below the deltoid insertion because the residual length is relatively long. The disability rate is different despite the same humeral amputation because the function of the amputated limb and post-prosthesis fitting differs considerably according to the residual length. The disability rate of a hand amputation is accepted as 90% if all fingers are amputated at the level of the metacarpophalangeal joint, but the disability rate is accepted as 54% if the thumb still remains because the function of the thumb is important. On a thumb amputation, the disability rate of an amputation at the level of carpometacarpal joint, metacarpal bone, metacarpophalangeal joint and interphalangeal joint are considered to be 38%, 37%, 36%, and 18%, respectively. A lower disability rate (the disability rate of distal amputation) is applicable if the amputation is performed between the standard levels because the functional difference is reduced by the development of prosthesis and the disability is reduced using various supporting instruments. On the other fingers, the same disability rate is applicable in an amputation of the 2nd and 3rd finger, and the same disability rate is applicable in an amputation of the 4th and 5th finger according to the importance of each finger. On the 2nd and 3rd finger, the disability rate of an amputation at the level of the metacarpophalangeal joint, proximal interphalangeal joint and distal interphalangeal joint are 18%, 14%, and 8%, respectively. On the 4th and 5th finger, the disability rate of an amputation at the level of the metacarpophalangeal joint, proximal interphalangeal joint and distal interphalangeal joint are 9%, 7%, and 5%, respectively. Table 1 gives a summary of the disability rates.
The disability of joint contracture
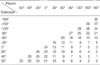
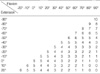
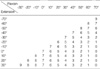
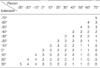
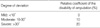
A disability originating from joint contracture occurs frequently after healing of the disease or trauma, and remains in most lesions of the upper limb after healing regardless of the cause. Therefore, it is very important to examine joint contracture when evaluating a disability of the upper limb. However, a proper evaluation of the small and various joint contractures is difficult. For a proper evaluation of joint contracture, the anatomical knowledge must be sufficient and the normal direction and range of motion of the joint need to be known. A measurement of joint contracture must be performed using a goniometer as follows. The joint contracture is divided into complete and partial contracture. Complete contracture is the case of a motionless joint with a range of motion of 0°. Partial contracture is the case of decreased joint motion and is evaluated from the starting point of motion in both directions. Both directional measurements must be carried out because the longitudinal and transverse axis of the described table of joint contracture are the starting and end points of joint motion, respectively. The method for measuring the disability rate originating from joint contracture is explained in the case shown in the table (Table 2) for extension-flexion contracture of the shoulder joint. The disability rate of the upper limb is 20% if the shoulder joint is fixed to 60° without any motion. -60° extension corresponds to flexion 60° at the table below and the crossover point of -60° extension of the longitudinal axis. 60° flexion of the transverse axis has a 20% disability rate of 60° fixed complete contracture. If the shoulder joint has extension-directed motion, even though there is no flexion-directed motion, it is a partial contracture and the disability rate decreases sequentially 20%, 13%, 12%, 11%, and 10% depending on the degree of extension-directed motion at the longitudinal axis. The disability rate is 13% if the shoulder joint has extension-directed motion from 60° to 30° flexion because it is 60° flexion and -30° extension. The disability rate is 11% if the shoulder joint has an extension-directed motion from 60° flexion to 0° flexion (neutral position) because it is 60° flexion and 0° extension. On the other hand, it is partial contracture if the shoulder joint has flexion-directed motion even though it has not extension-directed motion, and the disability rate decreases sequentially 20%, 18%, 16%, 13% and 12% depending on the degree of flexion-directed motion at the transverse axis. The disability rate is 18% if the shoulder joint has flexion-directed motion from 60° flexion to 90° flexion because it is -60° extension and 90° flexion. A lower disability rate (large joint motion) is applicable if the motion is between the degrees shown in the table. However, medium rate is applied if the difference between the disability rates is >4%.
Shoulder
The normal range of motion of the shoulder joint are 0-180° flexion, 0-50° extension, 0-180° abduction, 0-90° internal rotation and 0-90° external rotation. The measurement is performed with the patient sitting comfortably. The internal and external rotation are measured with 90° abduction of the shoulder joint and 90° flexion of the elbow joint. The disability rate of each extension-flexion, adduction-abduction and internal rotation-external rotation is determined by their tables, and the disability rate of the shoulder joint is determined by summing the individual contributions (Table 2, 3, 4).
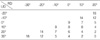
Elbow
The normal range of motion of the elbow joint is 0-140° extension-flexion, 0-80° pronation and 0-80° supination. The measurement is performed in the comfortably seated position. Pronation and supination are measured with 90° flexion of the elbow joint. The disability rate of each extension-flexion and pronation-supination is determined by their tables, and the disability rate of the elbow joint is determined by summing the individual contributions (Table 5, 6).
Wrist
The normal range of motion of the wrist joint is 0-60° extension, 0-60° flexion, 0-20° radial deviation and 0-30° ulnar deviation. The disability rate of each extension-flexion and radial-ulnar deviation is determined by their tables, and the disability rate of the wrist joint is determined by summing the individual contributions (Table 7, 8).
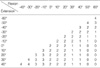
Hand
When measuring the range of motion of hand, 1) the wrist should be positioned at the neutral position and the forearm should be positioned at the pronation position, and 2) the other joints except the measuring joint should be positioned at the neutral position. For the expression of the range of motion, the neutral position is marked 0. Extension is marked (-) if the motion is directed towards flexion and (+) if the motion is directed towards extension. Flexion is marked (+) if the motion is directed toward flexion and (-) if the motion is directed towards extension. Hyperextension is generally admitted in the hand joint. For example, the normal range of motion of the metacarpophalangeal joint of the thumb ranges from 40° extension to 60° flexion. It is marked from 40° to -60° if it is expressed with extension and -40° to 60° if it is expressed with flexion. Therefore, extension 30° and flexion -30° mean the same angle and the cross point between transverse flexion 30° and longitudinal -30° corresponds to the complete ankylosis of flexion 30° (extension -30°). If measuring the range of motion is difficult, such as adduction of the thumb and opposition, the distance between 2 points is measured instead. There are many finger joints in the hand, and multiple contractures of the fingers are common after a fracture. However, the disability rate of each finger joint is lower than the shoulder or elbow. Therefore, the disability rate is <1% if it is calculated as the total disability of the upper extremity, and it may be an inappropriate evaluation because the disability rate is not adjusted accurately. Therefore, another disability rate is used for the hand, which is corrected to the disability rate of the upper extremity after summing the individual contributions from the other joints. The different disability rates of the same finger are combined. Regarding the method of summing, the summed rate (%) of a disability is calculated by the formula, (A+(100-A)×B/100), if each disability rate is A (%) and B (%). The disability rates of different fingers are simply added and the method for calculating the rate is (A+B) % because the function of the hand (100%) is divided into the thumb (40%), index (20%), middle (20%), ring (10%), and little finger (10%). This is converted to a disability rate of the upper extremity if the disability rate of the hand is multiplied by 0.9 and rounded up because the function of the hand is 90% of the upper extremity based on a disability from amputation (Table 9, 10). Care must be taken while summing the disability rates listed in the table below for the disability rate of a contracture of the hand because they are the disability rates for the hand.
Contracture of thumb
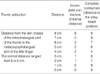
There are 1) flexion-extension motions of the metacarpophalangeal joint, 2) flexion-extension motion of the interphalangeal joint, 3) radial adduction-abduction, 4) adduction of the thumb, and 5) opposition of the thumb in the motion of the thumb. The contracture of radial abduction-adduction of the thumb is calculated by measuring the angle between the 1st and 2nd metacarpal bone. The radial abduction angle is determined by the maximal abduction of the thumb from the 2nd metacarpal bone. The normal range of motion of radial abduction is 0-50° because radial abduction is 0 when the thumb is maximally adducted to the 2nd metacarpal bone. Radial adduction is marked with (-) in the case of radial abduction (Table 11). Some points of the hand are used to calculate the disability rate of an adduction of the thumb because it is difficult to measure the angle of adduction directly. In the case of trauma to the hand, the thumb is frequently ankylosed to the adducted position. Therefore, it is possible to adjust the contracture of adduction of the thumb (Table 12). In case of contracture of the hand with the opposed position, the opposed contracture of the thumb is calculated from the distance between the skin crease of the interphalangeal joint and the distal palmar crease, such as below the finger, because the functional impairment of the hand is significant (Table 13).
Finger
The normal range of motion of the extension-flexion of metacarpophalangeal joints are 0-90° if the neutral position is extension 0°. However, the metacarpophalangeal joint requires hyperextension, and it has been suggested that hyperextension up to 20° is within the normal range. Contracture of the hyper-extended position and in cases where it is not possible to hyperextend must be considered an additional disability. The function of the index and middle finger are the same, the function of the ring and little finger are the same, and the function of the ring and little finger is 50% of the index and middle finger. The table shows the disability rate of each finger (Table 14, 15, 16, 17, 18, 19).
The disability according to the each disease
The disability according to each disease can be adjusted in the case of arthroplasty, instability, frequent dislocation and deformity in the shoulder, elbow, and wrist. A disability of contracture must be adjusted if the above mentioned diseases and contracture of the joint exist concomitantly. However, a disability according to each disease is adjusted if the measurements of the range of motion are inaccurate or the disability according to each disease is greater than the disability of contracture. The following rules must be obeyed if there are concomitant disabilities to avoid overlap of the grade of disability. The displacement of the joints in the finger, wrist, and elbow includes lateral deviation, rotational deformity (finger), and complex pathologies of these, such as subluxation or dislocation. These disabilities cannot be summed and only the greatest disability is accepted. The limitation of the disability rate of the shoulder, elbow, wrist and hand are 60%, 70%, 60%, and 90%, respectively. The maximal disability rate for each joint is the maximal disability of complete ankylosis.
Arthroplasty
The disability rate of arthroplasty is explained. An associated disability of contracture must be calculated individually and cannot be summed with arthroplasty. In addition, instability, subluxation, and dislocation after arthroplasty cannot be summed either. However, re-operation is recommended but may be impossible due to heart disease etc. if the symptoms are severe after the failure of arthroplasty (symptomatic failure or subluxation). In these circumstances, the maximal disability rate of a joint can be given. Arthroplasty is divided into replacement arthroplasty and resection arthroplasty, and the disability rate is adjusted according to the location of arthroplasty using Table 20. For example, the disability rate of the upper extremity is 24%, and the disability rate of a limitation of motion is 16% if flexion, extension, radial deviation, and ulnar deviation are 30°, 20°, 0°, and 30° after wrist replacement arthroplasty (radiocarpal and distal radioulnar joint), respectively. The final disability rate is 24% due to wrist replacement arthroplasty, which is greater, because the disability according to the each disease cannot be combined with a limitation of motion.
Instability
The disability rate is adjusted if instability has occurred after trauma to the upper extremity or disease. Instability means a subluxation or dislocation and can be combined with pain or functional impairment, and it should demonstrate objectively using a radiologic examination. The disability rate differs according to the degree of instability, and the severity of instability is divided into mild, moderate and severe. A mild degree is a situation where a perfect manual reduction is possible. A moderate degree is where perfect reduction is impossible using a manual reduction. A severe degree is a situation where a reduction is impossible. Table 21 shows the disability rate of each joint due to instability.
Dislocation
A disability from dislocation is adjustable but this dislocation is permanent. A dislocation and limitation of motion are frequently combined but a disability due to contracture and dislocation cannot be summed. The severity of the dislocation is divided into mild, moderate, and severe degree. The mild degree is a situation where perfect manual reduction is possible. A moderate degree is a situation where perfect reduction is impossible using a manual reduction. A severe degree is a situation where reduction is impossible. The disability rate of the upper extremity due to dislocation follows (Table 22).
Deformity
A disability from a deformity is adjusted if there is a deformity that is not evaluated with a disability of contracture or according to each disease. The disability is adjusted from 10% to 30% according to the severity of the amputation rate of each joint. There may be several deformities in the joint and bone of the upper extremity and hand after trauma or disease. However, it must be evaluated as a disability of contracture and with the following described deformity if combined with a disability of contracture. A disability of the lateral deviation of the finger is adjusted if there is lateral deviation without another disability. The disability is admitted if the lateral deviation of the hand is more than 10°, and the disability rate is calculated by multiplying the relative coefficient by the disability rate of an amputation of the finger. The disability rate of an amputation is based on the metacarpophalangeal joint, and the disability rate of the thumb, index and middle finger, and ring and little finger are 36%, 18%, and 9%, respectively. The disability rate of a lateral deviation of the finger cannot be combined with a disability of contracture in the same finger (Table 23). A rotational deformity of the finger is due to a mal-alignment of the metacarpal bone or interphalangeal joint after a fracture or joint unbalance (pronation of the index finger) after rheumatoid arthritis. A rotational deformity of the distal, middle, and proximal interphalangeal joint is calculated from the maximal active flexion of the finger. A mal-alignment of pronation or supination of the finger influences the function of the finger, and the disability rate is calculated by multiplying the relative coefficient of the degree of rotation by the disability rate of an amputation of the metacarpophalangeal joint. The disability rate of a rotation of the finger cannot be combined with a disability of contracture in the same finger (Table 24). A deviation of the wrist and elbow is also calculated as a disability. The radial and ulnar deviation of the wrist and elbow are calculated in the maximally extended position. The degree of lateral deviation is compared with the normal contra-lateral side, and the wrist and elbow are evaluated based on 0° and 15°, respectively, if a comparison with the contra-lateral side is impossible. The severity is divided into mild, moderate, and severe according to the degree of deviation. The disability rate is calculated by multiplying the relative coefficient by the maximal disability rate (Table 25).
The disability of muscle power
The disability rate is adjusted if there is definite weakness of the muscle and functional decrease in the upper extremity due to a substantial cause, and the cause of the muscle weakness should be described. In addition, it should not be a disability of contracture and according to each disease. A disability of muscle power includes the post-operative status after tendon-ligament rupture, compartment syndrome without a neurovascular injury, and muscle weakness after bone loss. The muscle weakness due to a nerve injury should be dealt with as a disability of the nerve. Subjective muscle weakness caused by pain is not included. The evaluation should be performed at the point of maximal medical improvement after treatment, at least one year after the trauma. An evaluation is carried out in the hand, elbow, and shoulder. The grip and pinch test are used to evaluate the hand and forearm. A manual muscle test is used to evaluate the elbow and shoulder. In the case of ipsilateral disease, the coefficient of power loss is used (normal power-limited force/normal force=coefficient of power loss %) to evaluate the hand. The coefficient of power loss is calculated using the average for Koreans if there is disease in the bilateral side or a difficulty in calculating the power of the healthy side (5). For grip measurements, in the sitting position, the arm is abducted 0°, the elbow is flexed 90°, and the wrist is neutrally positioned. A Jamar power goniometer is used and most comfortable position is chosen. The measurements are performed three times and the average is used. However, the disability is admitted if the deviation is less than 20%. The pinch power is measured with a lateral pinch among the chuck or three-digit pinch, key or lateral pinch and tip pinch with separate digits. The measurements are performed three times and the average is taken. The average measurement is compared with the average for Koreans if there is disease in the bilateral side. The difference according to gender is admitted but the difference according to occupation is not (Table 26). The shoulder and elbow are examined using a manual muscle test (MMT), and the loss of power in the wrist, elbow, and peri-shoulder muscle are evaluated. The disability of muscle power is MMT 3 or 4 degree. An anatomical injury should be found in case of MMT 0, 1, and 2, and the causative disability should be evaluated. A disability of muscle power should be evaluated as MMT 3 if no anatomical injury is found, and should be adjusted as a disability of muscle power. The disability of muscle power is not summed and only added (Table 27).
The disability of sensation of hand
The sensory nerve of the hand plays an important role in the hand functions that require micro-motion. A permanent functional loss of the hand is suspected in the case of crushing injury to the hand, long term disuse after surgery, and scar contracture that decrease the sensation. A peripheral nerve injury that is evaluated objectively using electromyography or a physical examination is included in the disability of nerve because the disability of hand sensation means a functional loss of the digital nerve. A pure sensory loss of the digit should be evaluated individually in a disability of hand sensation during an evaluation of the disability of the upper extremity, and it can be combined with a disability of the upper extremity function. An evaluation of the sensory loss of the finger is evaluated using a two point discrimination test or a sensory nerve examination. The sensory loss using a two point discrimination test is evaluated as sensory loss if less than 15 mm can be discriminated. The disability rate of sensory loss of the digit depends on the importance of the sensory nerve for each digit. The disability of each digit can be summed. A transverse disability means sensory loss in the medial and lateral side of the digit, and a longitudinal disability means sensory loss in the medial or lateral side of the digit (Table 28). The disability rate of each digit is not summed and only added. The entire sensory disability is summed with the other disabilities in the upper extremity using the following formula, (A%+(100-A)×B%).
The disability of the vessel
A disability of the vessel of the upper extremity means a peripheral vessel disorder of the artery and vein, and is evaluated with the functional impairment due to Reynaud's phenomenon. A disability due to the lymph edema can be adjusted to a disability of the vessel according to the severity of symptoms. Reynaud's phenomenon must follow a pallor, cyanosis, and purpura. It must not be judged as Reynaud's phenomenon if there is pain or the fingers show pallor, and it should not be admitted as a disability of the vessel. A disability of the vessel is admitted only if a radiologic examination shows abnormal findings, and should be associated clinical symptoms with decreases in function. There are some clinical symptoms (limping, pain at rest, and edema), and an evaluation of the disability should be performed after confirming the obstruction by using Doppler or nuclear examination. There is a disability of the vessel if the ratio between the arterial finger pressure and the pressure of the upper arm is <0.8 in the involved finger, even though Reynaud phenomenon is absent. The method of evaluation is graded according to the symptoms and examination results, and the disability rate is adjusted. A disability of the vessel cannot be summed with other disabilities. A disability of amputation is adjusted if the amputation is performed due to peripheral vascular disease. However, a disability of the vessel is adjusted if it is greater than the disability from an amputation (Table 29). The lymph edema is evaluated as a disability if the lymphangiogram is decreased using in the scintigraphy, and it is classified as mild, moderate, and severe. A mild degree is lymph edema grade 1, which shows a circumferential difference <2 cm and there is no disability. A moderate degree is lymph edema grade 2, which shows a circumferential difference >2 cm and requires continuous elastic support, and it is adjusted to a grade 2 vessel disability. A severe degree is lymph edema grade 3, which shows a circumferential difference <5 cm, and has disability in the daily activities but no other disability, and it is adjusted to a grade 3 vessel disability.
DISCUSSION
An evaluation of a disability of the upper extremity requires a delicate examination. Therefore, it is believed that the AMA guideline is more rationale than McBride. However, the AMA guideline has considerable contents and an adjustment in a clinic is difficult. Furthermore, it is not profitable because it involves a subjective evaluation for compensation purpose (1). This proposal has not overcome the AMA guideline. However, it has combined following advantages of the two methods. First, the field of disability is limited by 6 departments. Second, the table of an evaluation of joint motion is suggested as a format of McBride, which a domestic board are accustomed to. Third, an interval according to the contracture of the joint is established in order to reduce the conflict between the passive and active range of motion. Fourth, a subjective evaluation, such as a pain, is not performed and the intergrade difference of sensation and muscle power can be determined subjectively compared with the AMA guideline. Pain cannot be excluded entirely because it causes an obvious disability and functional impairment even though it is subjective. Therefore, this proposal compensates for this using the contracture of the joint and muscle power. The 6 departments are a sum of an evaluation with other assessments of a disability because a duplicated disability with the upper extremity should not be admitted if a disability of pain is associated with nerve impairment. This proposal has scientific and objective merit, and gives importance to a comfortable evaluation. Compared with the AMA guideline, this proposal is somewhat simple but there is a complex aspect because of the delicate features of the upper extremity. Therefore, the comfortable aspects and utility of this proposal must be demonstrated in clinics. Continuous feedback must be given to delete the unnecessary portion and add an insufficient portion by a suitable board. In addition, grading is needed and generality must be maintained considering the equality with the musculoskeletal system of the lower extremity, heart, lung, and other organs. A step is needed to evaluate labor impairment, considering the occupational ability and a compensation object. The impairment of daily activity and labor ability must be considered after taking the complexity of the upper extremity function into account. Social consensus must be achieved for an objective evaluation and the inter-departmental consensus is the first step for social consensus. Therefore, this proposal is a great advancement in evaluating disabilities.




















 XML Download
XML Download