

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Although we have used several systems for the evaluation and the compensation of the physical impairment patients in Korea, none of them is considered to be good enough to meet the high standard of requirement of the courts, the medical community and workers' compensation authorities (1-3). Furthermore as these are from other countries, they could not reflect the condition of Korean people (4).
In the urinary and reproductive systems of current Korean welfare act for the disabled, only the patients with hemodialysis or peritoneal dialysis due to chronic renal failure and the patients with transplanted kidney and the patients with urinary diversions are acknowledged as the disabled (3). A lot of patients could not get compensatons because the law doesn't cover them. Besides, the compensation of the disability requires different forms of medical certificate for each standard with further inconvenience.
In the United States of America, there is a scientific guideline to the evaluation of permanent impairment, established by American Medical Association (AMA) (2). Also, new version of AMA guideline was published in 2007 (5).
Therefore, it is about the time we had a new evaluation system which is not only scientific and useful, but appropriate to the culture and condition of Korean people as well.
The purpose of this report is to describe the resolved criteria of Korean Academy of Medical Sciences (KAMS) committee on a permanent impairment in urinary and reproductive systems, in assessing the severity and in determining the impact of the impairment on the ability to perform daily activities. But this is a preliminary report. A lot of part can be revised through future studies.
MATERIALS AND METHODS
In March 2007, KAMS planned a project for new evaluation of permanent impairment for Korean. It organized 11 committees for each organ and asked them to make new systems on the evaluation of the permanent impairment (6). The committee of genitourinary system consisted of ten physicians who were recommended by Korean Association of Internal Medicine, Korean Urological Association and Korean Society of Obstetrics and Gynecology.
Through two workshops, the members of the committee were informed of the background, purpose, basic concept and rating methods of impairment rating guideline. The evaluation systems for the permanent impairment of European Union, the United States or some countries in Asia (7) were also reviewed.
Especially, the AMA Guideline 5th edition (4) on the evaluation of permanent impairment made a good reference. Also, 6th edition of the AMA Guideline (5) is published in 2007. Nevertheless, we tried to make our own one which would accommodate the culture of Korean people.
An impairment is considered permanent when it has reached Maximal Medical Improvement (MMI); the impairment is nearly well stabilized and it is unlikely to change in the next year with or without medical treatment. Furthermore, the evaluation for the permanent impairment should be done when a patient reaches MMI. (5)
This evaluation guides for genitourinary system consist of four parts; upper urinary tract (kidney), lower urinary tract (bladder & urethra), male reproductive systems including prostate, and female reproductive systems.
RESULTS
Guideline for evaluation of upper urinary tract impairment (Table 1)
Kidney plays important roles in excretion of metabolic waste, acid-base balance, control of blood pressure (BP), and erythropoietin production. Serum creatinine (Cr) and creatinine clearance rate (Ccr) account for renal function and are useful to measure upper urinary tract function. Renal impairment is evaluated by medical nephrologist and pediatric nephrologist.
Laboratory findings
Either Serum Cr or Glomerular Filtration Rate (GFR) is used. Based on optimal results, GFR evaluation method is assessed by medical and pediatric nephrologists.
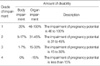
Disorder grade (Table 1)
Disorder is graded by renal function test, kidney transplantation, dialysis etc.
In case of different results between serum Cr and GFR, the poorer renal function is selected.
Impairment grade is assessed in MMI because of the possibility of disease progression or improvement.
Hemodialysis longer than 3 months due to chronic renal failure (CRF) is recognized as first grade, and kidney transplantation is recognized as third grade. According to the function of transplanted kidney, it can be recognized as more severe grade.
Patients on hemodialysis reach MMI at 3 months after the start of the treatment. Patient with kidney transplantation reaches MMI in 6 months after the surgery. On condition that there is no rejection symptom and a physician decides that the kidney function becomes stabilized. When a patient gets kidney transplantation after hemodialysis, MMI is reached at 3 month after the beginning of the dialysis and the impairment rating should be done in 6 months after the operation.
When children are evaluated, disability rate is added by 10%.
Guideline for evaluation of lower urinary tract impairment (Table 2)
Lower urinary tract impairment is evaluated by urologists.
Guideline for lower urinary tract impairment evaluation
The bladder is a urine reservoir that is voluntarily controllable. Normally it permits several hours of urinary retention. Pathologic conditions within or outside the urinary system may induce bladder dysfunction.
In women, the urethra is a urinary passage and has a voluntary sphincter, but no circular smooth muscle sphincter. In men, the urethra has a voluntary sphincter and propulsive muscles, and is a passage for urine and seminal ejaculations.
Symptoms and signs
Urinary frequency, dysuria, urinary incontinence, urine retention, hematuria, pyuria, passage of urinary calculi, suprapubic mass, diminished urinary stream, extraneous or ectopic urinary openings, periurethral masses, etc.
Disorder grade
Grade of lower urinary tract impairment would be determined according to Table 2.
Impairment grade is assessed in fixed or stable impairment without disease progression or improvement.
The findings of urodynamic study are not considered in lower urinary tract impairment evaluation.
Guideline for evaluation of male reproductive organ impairment
The male reproductive organs include the penis, scrotum, testicles, epididymis, spermatic cords, prostate, and seminal vesicles. The percentages would be increased by 50% for men younger than 40 yr, and decreased by 50% for men older than 65 yr.
The impairment of male reproductive organ impairment is evaluated by urologists.
Guideline for evaluation of penile impairment (Table 3)
The penis has the sexual functions of erection and ejaculation. Urinary function of the penis is discussed before. When evaluating the impairment of penis, consider impairment of both sexual and urinary functions. Impairment of sexual function would be determined according to Table 4. To determine impairment of the whole person, this estimate would be combined with the appropriate percentage for estimated urinary function impairment. This classification also may be used to estimate penile implant impairment.
Symptoms and signs
Erection and sensation abnormalities of the penis, partial or complete loss of the penis, etc.
Disorder grade
Objective techniques useful in evaluating penis function include, but are not limited to, penile tumescence studies, doppler ultrasound penile blood flow evaluations, dynamic cavernosometry, cavernosography and angiography. (8)
Disorder is graded by the degree of vaginal penetration, erection, ejaculation and orgasm using international index of erectile function (IIEF) questionnaire, nocturnal penile tumescence (NPTM) and color doppler ultrasonography (CDU).
Guideline for evaluation of scrotum impairment (Table 4)
The scrotum covers, protects, and provides a suitable environment for the testicles.
Symptoms and signs
Pain or enlargement of scrotum, testicular immobility, inappropriate testicle location, testicular masses, etc.
Disorder grade
Objective techniques useful in evaluating scrotum function include, but are not limited to, observation, palpation, testicular examination, and scrotal ultrasound. (9)
Disorder is graded by scrotal pain or discomfort, architectural alteration of scrotum, the state of testicular function and the location of testicle.
Guideline for evaluation of testis, epididymis and spermatic cord impairment (Table 5)
The testicles produce spermatozoa and synthesize male steroid hormones. The epididymis and spermatic cords transport the spermatozoa.
Symptoms and signs
Local or referred pain, tenderness and change in size, contour, position, and texture, testicular hormones and seminal fluid abnormalities, size and textural changes, testicular, epididymal, and spermatic cord function disturbances, etc.
Disorder grade
Objective techniques useful in evaluating testicular, epididymal, and spermatic cord function include, but are not limited to, vasography, ultrasound, spermatic arteriography and venography, biopsy, semen analysis, and clomiphene stimulation test, gonadotropin releasing hormone (GnRH) stimulation test, and human chorionic gonadotropin stimulation test (9).
Disorder is graded by testicular symptoms or signs, architectural alteration of testis, epididymis or spermatic cord, the need of continuous treatment, analysis of semen or hormone.
The solitary testicle is recognized as third grade.
Guideline for evaluation of prostate and seminal vesicle impairment (Table 6)
The prostate and seminal vesicles provide the appropriate nutrition, environment, and transport for spermatozoa and semen. Impairments associated with urinary functions of the parts of the urethra involved with the prostate are discussed in the lower urinary tract system.
Symptoms and signs
Local or referred pain, tenderness, oligospermia, hemospermia, urinary tract abnormalities, etc.
Disorder grade
Objective techniques useful in evaluating prostate and seminal vesicle function include, but are not limited to, urography, endoscopy, prostatic ultrasonography, vasography, biopsy, prostate secretion examination, magnetic resonance imaging (MRI), and hormone excretion pattern analysis (10).
Disorder is graded by the function of prostate and seminal vesicle, symptoms or signs related to prostate and seminal vesicle disease and the need of continuous treatment.
Sexual dysfunction or urinary incontinence by radical prostatectomy to treat prostatic cancer is recognized as first grade.
Guideline for evaluation of female reproductive organ impairment
The female reproductive organs include the vulva, vagina, cervix, uterus, fallopian tubes, and ovaries. Impairment of female reproductive organs is strongly influenced by ovarian function which changes with aging. Physiologic changes, before and after menopause, are very important when evaluating and estimating female reproductive organ impairment.
Guideline for evaluation of fallopian tube and ovary impairment (Table 7, 8)
The Fallopian tubes transport ova, and spermatozoa. The ovaries develop and release ova and secrete sex and reproductive hormones.
Symptoms and signs
Vaginal bleeding or discharge, fallopian tube stenosis or obstruction, abnormal morphologic characteristics, pelvic masses or neoplasia, absent, infrequent, or abnormal ovulation, abnormal hormone secretion, menstrual dysfunction, etc.
Disorder grade
Objective techniques useful in evaluating fallopian tube and ovarian function include, but are not limited to, cervical and vaginal cytologic smears, pelvic roentgenography, hysterosalpingography, ovarian biopsy, blood and urine hormonal assays, ultrasonogram, computed tomography, magnetic resonance imaging, laparoscopy, and basal body temperature studies.
Disorder is graded by symptoms or signs related to vulva or vaginal disease, the need of continuous treatment, the possibility of delivery or sexual intercourse.
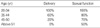
The degree of impairment is modified according to age (Table 9).
Guideline for evaluation of uterus and cervix impairment (Table 10)
The most important function of uterus is to maintain pregnancy. Impairment of uterine corpus and cervix may have an effect on the maintenance of pregnancy. Because maternal age is also an important factor for pregnancy, it is strongly recommended to consider in assessing uterine function. In this part, we excluded fertility disadvantage related to ovarian function which is shown by menstrual dysfunction. Uterine impairment is confined to organ impairment rate. Diagnostic tools for assessing uterine impairment are listed in Table 11.
We calculated final uterine impairment by multiplying the rate of age-related uterine impairment and the rate of diseaserelated uterine impairment (Table 12).
Symptoms and signs
Women with uterine impairment do not show specific symptoms and signs. Most of them visit a hospital due to menstrual dysfunction and infertility. The others are women who experienced hysterectomy because of uterine myoma or cancer.
Disorder grade (Table 10)
Disorder is graded by percentage of pregnancy potential.
Disorder is graded by percentage of pregnancy potential.
If women have more than one morbid conditions of uterus, the sum of the rate of disease-related uterine impairment is considered as her total impairment rate. When it exceeds 100%, 100% is considered as her total diseases-related uterine impairment rate. The only exception is a case of hysterectomy. In this case, 100% impairment is assigned regardless of women's age.
If the degree of uterine impairment is changed (for example, in cases of hysterectomy, septostomy, or adhesiolysis), it should be reassessed.
Guideline for evaluation of female external genitalia impairment (Table 13, 14)
The vulva has cutaneous, sexual, and urinary functions. Urinary function is discussed in the urinary system. The vagina has a sexual function and also serves as a birth passageway. The clitoris is an erectile organ that has an important role in sexual functioning.
Symptoms and signs
Sensation alteration or loss, lubrication loss, partial or complete absence of vulva and vagina, vulvovaginitis, vulvitis, vaginitis cicatrization, ulceration, stenosis, atrophy or hypertrophy, neoplasia or dysplasia, difficulties with sexual intercourse, urination, or vaginal delivery, underlying perineal structure support defect, etc.
Disorder grade
Vulvar and vaginal impairment evaluation is divided into two guides in terms of delivery or sexual function.
Disorder is graded by symptoms or signs related to vulvar or vaginal disease, the need of continuous treatment, the possibility of delivery or sexual intercourse.
The degree of impairment is modified according to age (Table 9).
DISCUSSION
In the United States, the American Medical Association's Guides (4) to the evaluations of permanent impairment have been developed and are the most commonly used source for assessing and rating an individual's permanent impairment. Even though we referred the AMA's guideline 5th edition (4) as a model, we also tried to make our own which would fit more for Korean people.
Needless to say, the ideal evaluation of impairment should depend entirely on objective findings of the patients. However, the reality is different. We just try to use more objective tools in the evaluation. And physicians could determine the rating in a comprehensive way using subjective and objective findings. We are afraid that the determination of the rating would be somewhat different depending on physicians, especially in patients with voiding dysfunction and sexual dysfunction.
Evaluation of upper urinary tract system impairment
Originally, the first Korean version of the Guideline to the Evaluation of Permanent Renal Impairment (11) was based on the guideline similar to that published by American Medical Association (4). The revised second Korean version of the Guideline to the Evaluation of Permanent Renal Impairment offers several following features.
First, we simplified grading instructions to promote consistent scoring of impairment ratings and to minimize the bias among physicians. In the previous edition, grading system was complex and complicated.
We unify these three groups (Table 15) into one group (Table 1) with deleting relatively mild symptoms and signs, such as edema, hematuria or proteinuria and renal osteodystrophy. We also clarified the definition of symptoms and signs, such as "renal anemia" as hemoglobin ≤10 gm/dL and "severe hypertension" as diastolic blood pressure ≥110mmHg (12).
We changed methods for measuring renal function to Ccr and serum Cr level from blood urea nitrogen (BUN), Ccr and serum Cr level in the previous version. Serum Cr is the most widely used marker for GFR (13). BUN is affected by state of hydration, catabolism and liver disease. Ccr is a more accurate measure, however, there are many clinical settings where a Ccr is not available, and decisions concerning drug dosing must be based on the serum Cr. A formula that accounts for age-related decreases in GFR, body weight, and sex and allows an estimate of Ccr in men has been described by Cockcroft-Gault (12):

In children, creatinine clearance can be estimated by Schwartz formula (14):
Creatinine clearance (mL/min/1.73 m2)=κ×height (cm)/serum creatinine (mg/dL)
(κ: 0.55 for children and adolescent females, 0.7 for adolescent males)
We simplified grading instructions for physicians to judge grade by either renal dysfunction or symptoms and signs, but not by both of them.
Second, we extended three grades (Table 16, 17) into four grades (Table 1) to accommodate diversity of renal impairment. We place chronic dialysis patients into the first grade and renal transplant patients into the third grade.
Third, we added new guideline for pediatric patients with permanent renal impairment, because normal serum Cr and Ccr are different according to age or body surface area of pediatric patients. We also added criteria of severe hypertension in pediatric patients in "Symptom and Signs of Chronic Renal Disability" (Diastolic pressure in child ≥95 percentile of normal diastolic blood pressure of same age).
Evaluation of lower urinary tract system impairment
We developed a system with special attention paid to the following points.
First, impairment grades for bladder and urethral dysfunction is incorporated. This is based on the fact that not all impairments of the lower urinary tract could be objectively demonstrated. The sole use of strict objective criteria with numerical values has a high possibility of masking actual impairments as normal findings or vice versa. An appropriate combination of both objective and subjective results is incorporated in deciding the final impairment grade to better reflect the actual degree of impairment.
Second, changes to the upper urinary tract and use of urinary diversions are incorporated in the decision of an impairment grade.
Third, a number of causes of artifact in cystometry must be recognized. There are technical issues such as pressure measurement artifacts (the presence of air bubbles, kinked tubing, incorrect placement, migration of the pressure catheters) and infusion rate artifacts (especially in neurogenic bladder) and patient-related issues, including lack of cooperation, outlet incompetence, and vesicoureteral reflux. If the bladder outlet is incompetent, urine may leak around the filling catheter and a low bladder compliance may not be diagnosed because the bladder is never adequately filled (spinal dysraphism, severe intrinsic sphincter deficiency [ISD] in an older woman, etc) (15). In this scenario, cystometry may not be the main role in rating permanent impairment of lower urinary tract system. So the findings of urodynamic study are not considered in lower urinary tract impairment evaluation.
Evaluation of male reproductive system impairment
It is difficult to exactly evaluate the ratio of impairment of organ function induced by trauma or disease, because all dysfunctions are not exposed to outside of the body. The impact of erectile dysfunction would be greatly different depending on age, marital status and occupation, etc. Erectile dysfunction is less important in old ages than in young ages. For example, the penis is not vital organ and is not needed at work, but erectile function in young patients who are sexually active is very important. Therefore, in the guideline, we added the 50% of the score expected in patients under 40 yr old, whereas we substracted the 50% of the score expected in patients over 65 yr old. We hope that the evaluation of the genital organ impairment should be reevaluated in the future, since the living standard of Korean people is getting better.
In the guideline of impairment of genital organ function, some symptoms and signs are quantitatively evaluated by medical instruments, laboratory examinations or questionnaires, however, others would not be quantitatively evaluated by the same tools. Therefore, doctor's bias may distort the evaluation. In opposite view, some symptoms and signs are subjectively made by patients. Nevertheless, doctors can not deny patient's symptoms such as erectile dysfunction or orgasmic dysfunction.
Evaluation of male reproductive system impairment
Evaluation of female reproductive system impairment We revised the female reproductive system with special attention paid on the following points. First, impairment of female reproductive system function is influenced by age, especially women in child-bearing age. Therefore, we consider physiologic differences between premenopausal and postmenopausal women when evaluating and estimating female reproductive organ impairment.
Second, we tried to describe pregnancy rate according to ovarian or uterine diseases.
Third, we tried to express appropriate diagnostic tools to evaluate uterine impairment.
Fourth, we showed the rate of age-related loss of pregnancy potential and the rate of disease-related loss of pregnancy potential in terms of uterine impairment. Unlike AMA Guideline, therefore, we evaluated uterine impairment according to pregnancy potential. Fifth, we tried to divide the vulvar and vaginal impairment, into delivery and sexual function.
In conclusion, we tried our best to make this evaluation system objective, scientific, and convenient as much as possible. Nevertheless, we still find it to be revised much more. We hope that this would help many patients with impairment as well as doctors who evaluate them in the future.















 XML Download
XML Download