

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Coronary artery disease is usually caused by atherosclerosis and associated with traditional risk factors such as smoking, hypertension, diabetes mellitus, aging, and hyperlipidemia (1, 2). Besides these traditional risk factors, recently, several newer risk factors and surrogate markers for the early detection of atherosclerosis including the measurement of endothelial dysfunction, arterial wall structure, arterial stiffness, and serologic markers of vascular inflammation were proposed and widely had been studied (3, 4).
Endothelial dysfunction involves every stages of the progression of atherosclerosis (5, 6) and is non-invasively measured by flow-mediated vasodilation (FMD) of the brachial artery (7). Arterial stiffness is now an established cardiovascular risk factor and one of the best prognostic indicators for future events in hypertensive population. Pulse wave velocity (PWV) is a simple, reproducible, and non-invasive measurement which can be used as a valuable index of both arterial stiffness and atherosclerosis in large populations (8). Recent studies have been demonstrated that high sensitivity C-reactive protein (hsCRP) and microalbuminuria were significantly associated with the presence or severity of atherosclerotic cardiovascular diseases and could be used as simple surrogates of atherosclerosis (9-12).
In the previous studies, some kinds of drugs, although they had individual differences, such as angiotensin converting enzyme inhibitor (ACEI), angiotensin receptor blocker, or calcium channel blocker (CCB) could improve endothelial function and arterial stiffness, and decrease the level of hsCRP and microalbuminuria (13, 14). However, the effects of CCB mono-therapy and CCB plus ACEI combination therapy on these surrogate markers in patients with angina pectoris were poorly evaluated.
Therefore, the aim of this study was to evaluate the effects of CCB and ACEI on surrogate markers of atherosclerosis including endothelial function, arterial stiffness, urinary albumin excretion (UAE), and hsCRP in patients with angina pectoris.
MATERIALS AND METHODS
Study design
The study is a single-center, randomized, open clinical trial to evaluate the effects of CCB and ACEI on surrogate markers of atherosclerosis including endothelial function, arterial stiffness, UAE, and hsCRP in patients with stable angina pectoris (SAP). The study protocol was approved by the Institutional Review Board of Chonnam National University Hospital and informed consent was obtained from each patient. Inclusion criteria were 1) patients with newly diagnosed SAP who underwent coronary angiography for the first time, 2) diameter stenosis more than 50% of target lesion, 3) successful, uncomplicated percutaneous coronary intervention with less than 10% residual stenosis, 4) able to give informed consent, 5) able to successful follow-up measurement of FMD, PWV, UAE, and hsCRP. Exclusion criteria included 1) prior history of coronary intervention, 2) blood pressure more than 160 mmHg in systole and 100 mmHg in diastole, 3) known intolerance to CCB or ACEI, 4) previous use of angiotensin receptor blocker, 5) known heart failure or ejection fraction <50%, 6) renal insufficiency with creatinine >2.5 mg/dL, 7) need for warfarin anticoagulation, 8) known hepatic dysfunction, 9) current participation in another randomized trial, 10) major life threatening illness, 11) patients refusal during clinical follow-up or incomplete clinical follow-up.
Study subjects
From September 2004 to April 2006, a total of 92 patients with SAP were enrolled initially. Among them, 5 patients were excluded owing to the adverse events (intractable cough: 2 patients in group II, headache: 1 patient in group II, facial flushing: 1 patient in group I, follow-up loss: 1 patient in group I). Although dry cough was developed in 6 patient of group II, the symptom was not severe and tolerable in 4 patients and thus the study was continued except for 2 patients who complained intractable cough. Therefore, a total of 87 patients (57.6±10.0 yr, 52 males) were finished this study and analyzed. The patients were divided into two groups according to the treatment modalities with 1 to 1 fashion; CCB (cilnidipine 10 mg per day) group (group I: n=44, 57.9±9.7 yr, 23 males) and CCB (cilnidipine 10 mg per day) plus ACEI (captopril 25 mg per day) group (group II: n=43, 57.2±10.5 yr, 29 males). FMD, PWV, UAE, and hsCRP were compared at baseline and 6 months after treatment. All parameters were measured early in the morning following overnight fasting more than 12 hr. Vasoactive medications including long-acting nitrates or intravenous nitrates or CCB or ACEI were withheld and not prescribed for at least 24 hr until the baseline measurements were completed. Only short-acting sublingual nitroglycerin for control of angina and anti-platelet agents were permitted. The doses of CCB or ACEI were not changed during the study periods. Follow-up measurements were also preformed early in the morning after 6 months of medical treatment at more than 12 hr after last dosing.
Measurement of endothelial function
FMD of the brachial artery as the non-invasive parameter of endothelial function was measured according to the guideline described previously (7). A 8 MHz high resolution linear vascular ultrasound transducer was used to image the brachial artery longitudinally just above the antecubital fossa. The tourniquet measuring blood pressure was placed on the forearm in order to create shear stress induced by reactive hyperemia. The diameter of the brachial artery was measured at the onset of the R-wave on electrocardiogram. After baseline measurements of the brachial artery diameter, the blood pressure cuff was inflated to at least 50 mmHg above systolic blood pressure to occlude arterial flow for 5 min. Subsequent deflation of the cuff induces a brief high flow state through the brachial artery (reactive hyperemia) to accommodate the dilated resistance vessels. The resulting increase in shear stress causes the brachial artery to dilate. The brachial artery was imaged for the first 2 min of reactive hyperemia continuously. The flow-mediated dilatory response was used as a measure of endothelium dependent vasodilation. After the 10 min of rest to reestablish baseline condition, 0.6 mg of nitroglycerin was administered sublingually. The brachial artery was imaged for 5 min continuously to measure peak diameter. The dilatory response to nitroglycerin was used as a measure of endothelium independent vasodilation.
Measurement of arterial stiffness
Assessment of arterial stiffness was performed non-invasively with the commercially available VP-2000 PWV analysis system (Colins, Komaki, Japan). All PWV measurements were performed by the single well-trained clinical technician at supine position in a quiet, temperature controlled room after at least 10 min of rest. Heart-femoral and brachial-ankle PWV were measured and used for analysis. Brachial-ankle PWV were calculated from the mean value of the right and left brachial-ankle PWV.
Measurements of UAE and hsCRP
UAE was measured by turbidimetric immunoassay method using Olympus 5431 autoanalyzer in a spot urine samples by simultaneously assessing creatinine excretion (mg/g Cr), collected from the first voided mid-stream urine. The level of hsCRP was measured by immunoturbidimetric CRP-Latex (II) assay using Olympus 5431 autoanalyzer. The sample for the measurement of hsCRP was obtained early morning in overnight fasting more than 12 hr before coronary angiography or intervention.
Study endpoints
Primary endpoints were changes of FMD, PWV, UAE, and hsCRP at 6 months. Secondary endpoints were major adverse cardiac events including death, myocardial infarction, and target lesion revascularization during the study periods between the groups.
Statistical analysis
Statistical analysis was performed using commercially available software (SPSS for Windows, Version 13.0, Chicago, IL, U.S.A.). All parameters were expressed as the mean±standard deviation. Categorical variables were evaluated using chi-square test. Differences in the mean values between the 2 groups were evaluated using unpaired t-test and changes in the mean values using paired t-test. Numerical correlations were established by a Spearman correlation. A p value of less than 0.05 was considered to be statistically significant.
RESULTS
Baseline clinical characteristics
The study population consisted of 87 patients (57.6±10.0 yr, 52 males) with stable angina pectoris who had newly diagnosed coronary artery disease by coronary angiography. Baseline clinical characteristics including age, sex, risk factors, and prescribed medications were not different between the groups (Table 1).
Angiographic characteristics
Angiographic characteristics are summarized in Table 2. Baseline angiographic variables including target lesion, number of diseased vessel, types of implanted stent, lesion morphology, and severity of diameter stenosis were not different between the groups.
Baseline measurements of FMD, PWV, UAE, and hsCRP
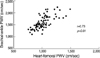
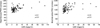
FMD of the brachial artery was 7.7±3.2% and nitroglycerin mediated vasodilation was 16.8±4.6%. Heart-femoral PWV was 1,020.3±146.1 cm/sec and brachial-ankle PWV was 1,604.3±277.9 cm/sec (right: 1,598.7±276.1, left: 1,609.7±285.6). UAE was 17.1±24.7 mg/g Cr and the level of hsCRP was 0.23±0.37 mg/dL. Heart-femoral PWV were significantly correlated with brachial-ankle PWV (r=0.73, p<0.01) (Fig. 1). UAE were significantly correlated with heart-femoral PWV (r=0.51, p<0.01) and brachial-ankle PWV (r=0.43, p<0.01) (Fig. 2). However, FMD and hsCRP were not correlated with PWV or UAE. FMD, PWV, UAE, and hsCRP were not different between the groups at baseline (Table 3).
Changes of FMD, PWV, UAE, hsCRP, and hemodynamic parameters
FMD, PWV, UAE, and hsCRP were measured in all patients after 6 months of medical treatment. FMD were significantly improved in group II (7.5±3.7 to 8.8±2.7%, p<0.001), but not in group I (7.9±2.7 to 8.2±2.8%, p=0.535) (Fig. 3). FMD was improved in 31 patients and not changed or decreased in 12 patients of group II. PWV were more decreased in patients with the improvement of FMD than in patients without improvement of FMD, but it did not reached statistical significance (hfPWV: -93.6±148.6 vs. -58.9±75.7 cm/sec, baPWV: -127.3±193.7 vs. -75.1±110.4 cm/sec, p=ns). Brachial-ankle PWV were significantly improved in both groups (1,621.3±279.4 to 1,512.1±225.0 cm/sec in group I, p<0.001, 1,586.8±278.5 to 1,434.5±200.5 cm/sec in group II, p<0.001) (Fig. 4). However, heart-femoral PWV were significantly improved only in group II (1,025.7±145.1 to 946.2±112.2 cm/sec, p<0.001), but not in group I (1,015.1±148.6 to 1,000.1±132.8 cm/sec, p=0.06) (Fig. 5). FMD was improved in 31 patients and not changed or decreased in 12 patients of group II. The improvement of FMD was not associated with the changes of PWV. UAE were significantly decreased only in group II (20.19±29.92 to 13.03±16.42 mg/g Cr, p=0.019), but not in group I (14.15±18.19 to 12.80±15.50 mg/g Cr, p=0.214). The levels of hsCRP were not changed in both groups (0.19±0.33 to 0.16±0.20 mg/dL in group I, p=0.307, 0.25±0.42 to 0.21±0.25 mg/dL in group II, p=0.111). Systolic and diastolic blood pressures were significantly improved in both groups, but were not different between the groups at 6 months. Heart rates were not changed in both groups and were not different between the groups at 6 months. Changes of FMD, PWV, UAE, hsCRP, and hemodynamic parameters were summarized in Table 3. FMD was improved in 31 patients and not changed or decreased in 12 patients of group II. The improvement of FMD was not associated with the changes of PWV.
Clinical events during follow-up periods
Clinical follow-up were possible in all patients. Death, myocardial infarction, or stent thrombosis was not developed in both groups. Follow-up coronary angiography at 6 months was performed in 55 patients (29 patients in group I, 26 patients in group II). Target lesion revascularization were performed in 5 patients (9.1%) due to restenosis and were not different between the groups (3 patients: 10.4% in group I, 2 patient: 7.7% in group II, p=0.763). Baseline and follow-up values of FMD, PWV, UAE, and hsCRP were not associated with angiographic restenosis.
DISCUSSIONS
The main finding of the present study is that the combination therapy with CCB and ACEI more effectively improves endothelial function, arterial stiffness, and UAE than CCB mono-therapy do in patients with stable angina pectoris. American College of Cardiology/American Heart Association 2002 update guideline for the management of stable angina recommended that ACEI should be used in most cases as a routine secondary prevention for patients with known coronary artery disease based on the results of the Heart Outcomes Prevention Evaluation trial (15). However, the precise beneficial mechanism of ACEI in angina pectoris was not elucidated. Several mechanisms such as anti-proliferative effects, hormonal/vascular effects and anti-atherogenic properties were suggested as a favorable role of ACEI. Although the major adverse cardiac events were not different between the groups, the results of this study also support that ACE inhibition plays a beneficial role in the management of stable angina pectoris by anti-atherogenic effects including improvements of endothelial dysfunction, arterial stiffness, and UAE.
Recently, several surrogate markers for the early detection of atherosclerosis including the measurement of endothelial dysfunction, arterial wall structure, arterial stiffness, and serologic markers of vascular inflammation were proposed and widely studied (3, 4). Recent studies suggested that these surrogate markers for atherosclerosis are associated with the presence of atherosclerotic coronary artery disease and also associated with future adverse cardiac events (8-12). To reduce the risk of death or disability associated with atherosclerotic coronary artery disease, therefore, early identification and therapeutic modification of risk factors or surrogate markers are important.
Endothelial dysfunction measured by FMD of the brachial artery is associated with the presence of coronary artery disease or the severity of the coronary artery stenosis or in-stent restenosis following percutaneous coronary intervention (16, 17). Some kinds of drugs such as ACEI, angiotensin receptor blocker, or CCB are known to have beneficial effects on endothelial function in the previous studies. Mancini et al. (18) reported that ACEI (quinapril) could improve endothelial function measured by invasive measurements of coronary diameter change in response to acetylcholine in patients with coronary artery disease. Anderson et al. (19) also reported that ACEI (quinapril) could improve endothelial function measured by FMD of the brachial artery in patients with coronary artery disease, but CCB (amlodipine) could not improve FMD. In this study, combination therapy with ACEI (captopril) and CCB (cilnidipine) showed significant improvement in endothelial function measured by FMD of the brachial artery in patients with coronary artery disease. However, CCB monotherapy did not improve FMD of the brachial artery. The results of this study and Anderson et al. (19) suggested that ACE inhibition may play more important roles in endothelial function than calcium channel blockade in patients with overt coronary artery disease. Although FMD of the brachial artery were improved only in combination therapy group, clinical events were not different between the groups. FMD of the brachial artery were not associated with in-stent restenosis in this study. However, Kitta et al. (16) and Patti et al. (17) reported that impaired FMD of the brachial artery was a significant independent predictor of late in-stent restenosis following percutaneous coronary intervention. To date, no prospective randomized clinical trial in large population has evaluated the relationship between endothelial dysfunction and in-stent restenosis. Thus, further clinical trials will be needed to elucidate the relationship between endothelial dysfunction and in-stent restenosis.
Arterial stiffness is now an established risk factor for premature coronary artery disease, peripheral vascular disease, and stroke (8). It is a single best prognostic indicator for future cardiovascular events in hypertensive population and also predicts adverse outcomes in patients with documented coronary artery disease (20-24). PWV is a simple, reproducible, and non-invasive measurement which can be used as a valuable index of both arterial stiffness and atherosclerosis in large populations. The results of the studies including Nigam et al. (25, 26) suggested that large conduit artery stiffness correlates significantly with FMD of the brachial artery. However, the results of this study failed to demonstrate the relationship between PWV and FMD of the brachial artery at baseline and after 6 months of medical treatment. Although the PWV was more decreased in patients who showed the improvement of FMD, it did not reached statistical significance. Life style modifications and pharmacological therapy could improve arterial stiffness measured by PWV. Long-term ACEI therapy has been shown to be superior to diuretics or beta-blockers in improving carotid, femoral, or radial arterial compliance and is marginally superior to CCB therapy as well (14). CCB as a mono-therapy or combination therapy with ACEI improved brachial-ankle PWV, but heart-femoral PWV was only improved in combination therapy with ACEI and CCB in the present study. This finding suggested that combination therapy with ACEI and CCB could have more favorable effects on cardiovascular disease or events than CCB mono-therapy. The reason why heart-femoral PWV and brachial-ankle PWV showed different response is not clear, but several possible mechanisms would have been involved. Firstly, the improvement of heart-femoral PWV in group II is possibly associated with the pleiotropic effect of ACEI such as the favorable impacts on the aortic wall endothelial function or components. ACEI is known to be decrease collagen content, fibrosis, and thus improve elasticity. Secondly, the improvement of heart-femoral PWV in group II is possibly caused by the simple hemodynamic change of BP. Although the change of BP did not showed significant statistical difference, the drop of BP in group II was about 3 mmHg more than in group I. Furthermore, ACEI showed different response on central aortic pressure according to the age group in the previous studies. According to the study of Morgan et al. (27), ACEI therapy, despite a relatively small effect on peripheral BP, showed a more beneficial effect on central BP in elderly patients with hypertension. We did not checked central aortic pressure in the present study, but the changes of central aortic pressure in group II might be significantly higher than the changes of peripheral brachial BP. Thirdly, the number of the subjects involved in this study is relatively small and thus it also may affect the result of the heart-femoral PWV.
HsCRP is an important surrogate marker for atherosclerotic coronary artery disease and associated with cardiovascular events in patients with documented coronary artery disease (9, 10). We want to evaluate the relationship between hsCRP and other surrogate markers for atherosclerosis, and also the effects of pharmacologic treatment with CCB or CCB plus ACEI on the level of hsCRP. Several studies demonstrated that the level of hsCRP were significantly associated with FMD of the brachial artery, PWV, and UAE and improved by pharmacological therapy (28-31). However, the level of hsCRP were not correlated with FMD of the brachial artery or PWV, or UAE and not changed with pharmacologic treatments in this study. The correlation among these surrogate markers has not been reported consistently in the previous studies (26, 32, 33). None of the surrogate markers provides highly sensitive and specific recognition of progressive atherosclerotic cardiovascular diseases and rather than these surrogate markers may have different supplemental action mechanism in the development of atherosclerotic coronary artery disease (33). Therefore, an attractive strategy has been to use a combination of these surrogates to better define the presence of early disease.
Microalbuminuria measured by UAE is also an important surrogate marker for atherosclerosis and predicts future cardiac events (11, 12). UAE was significantly improved after combination therapy with CCB and ACEI, but not after CCB mono-therapy in the present study. This finding support that the inhibition of renin-angiotensin-aldosterone system can retard or reverse microalbuminuria (34). Although the change of UAE was not compared between the groups, however, the baseline level of UAE was significantly lower in group I than in group II. Therefore, we cannot exclude that the lower changes of UAE in group I might be caused by the lower baseline level than in group II. Recently, Morimoto et al. (35) reported that CCB (cilnidipine) was associated with the improvement in UAE besides the improvement of brachial-ankle PWV. This study showed the same finding compared with the present study in that CCB could improve brachial-ankle PWV, but the effect of CCB on UAE was the opposite. Their study also had a limitation that only the small numbers of the study population was involved. Therefore, the effect of cilnidipine on UAE should be considerably re-evaluated by more large randomized controlled trial.
There are some limitations in this study. Firstly, the main limitation of this study was the relatively small sample size and thus some selection bias could present inevitably. Secondly, although the prescribed medications such as statins or beta-blockers were not different between the groups, these drugs also could affect diversely on FMD, PWV, and UAE. Thirdly, although the degree of the fall of BP did not showed significant statistical difference between the groups, the greater fall of BP in group II than in group I would have affect the greater improvement of endothelial function and arterial stiffness in group II than in group I. Therefore, the degree of BP change between the groups should be controlled at a similar degree in the study design by adding hydrochlothiazide as a placebo in group I. Fourthly, the dose of the used ACEI was fixed (25 mg per day) and thus not reached its full dose. It may not be sufficient to evaluate the effect of ACEI.
In conclusion, combination therapy with CCB and ACEI more effectively improve endothelial dysfunction, arterial stiffness, and microalbuminuria than CCB mono-therapy in patients with angina pectoris.





 XML Download
XML Download