

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Fungal endocarditis is an uncommon occurrence; its incidence was reported as 1.3 to 6% of infective endocarditis cases (1). Aspergillus species contributes to approximately 25% of all cases of fungal endocarditis, second to the Candida species in frequency. Several conditions predispose patients to Aspergillus infections including underlying cardiac abnormalities, prosthetic heart valves, indwelling central venous catheters, prolonged use of broad-spectrum antibiotics, and intravenous drug abuse (1, 2).
We present a case of Aspergillus endocarditis of a native valve, presenting as a femoral artery occlusion.
CASE REPORT
A previously healthy 35-yr-old male was admitted with right leg pain. Four months previously, he underwent a pericardiocentesis for a fever and massive pericardial effusion; no organism was found in the pericardial effusion. A precordial systolic murmur was heard during auscultation of the heart, and a right femoral artery pulse was not detected. The transthoracic echocardiography revealed severe mitral insufficiency with large mobile vegetations on the anterior and posterior mitral valve leaflets (Fig. 1A). The computed tomographic angiography showed an embolic occlusion of both common iliac arteries (Fig. 1B). The patient underwent emergency replacement of the mitral valve with a 29 mm prosthetic mechanical mitral valve (SJM masters series, St. Jude Medical, St. Paul, MN, U.S.A.), and bilateral ilio-femoral artery thromboembolectomy with a Fogarty catheter through both femoral arteries. Gross findings in the surgical field revealed 1.5×1.5 cm round irregular vegetations on the middle portions of both mitral valve leaflets. The patient recovered well during the immediate postoperative period. However, a right popliteal artery occlusion was found four day after surgery. We performed a right popliteal artery thrombectomy through a supragenicular approach.
On histology, a fungal lesion showing the characteristic findings of Aspergillus was found. Culture of the valvular tissue on Sabouraud dextrose agar confirmed the Aspergillus species (Fig. 1C, D). Anti-fungal medication was planned with intravenous amphotericin B for six weeks then oral itraconazole for 12 weeks. Therefore, we started intravenous amphotericin B (5 mg/kg/day).
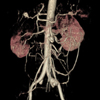
Forty days after the first operation, the patient complained of abdominal pain. A computed tomography showed multiple aneurysmal changes of the superior mesenteric artery (SMA), splenic artery, hepatic artery and left iliac artery despite amphotericin B treatment (Fig. 2). The patient underwent SMA aneurysmectomy and arterial reconstruction with bovine pericardium, and left iliac artery repair. Concomitant thromboembolectomy was performed because of the bilateral internal iliac artery occlusions. Amphotericin B was changed to oral itraconazole (800 mg/day) at 6 weeks after the first operation.
Fifty-eight days after the first operation, the patient had hematochezia, and had a colonoscopy that revealed multifocal intestinal bleeding. He recovered after massive transfusion and supportive care. The patient was discharged 78 days after surgery on oral itraconazole and warfarin. On follow-up, the itraconazole was discontinued 10 weeks later. He was alive and doing well 12 months later without recurrence. Unfortunately, he died in a traffic accident 13 months after discharge.
DISCUSSION
Aspergillus is a ubiquitous mold capable of causing several diseases in both healthy humans and immunocompromised hosts. Aspergillus species endocarditis is an ominous condition and its prevalence is increasing in the hospital population. Men are more commonly affected than are women with a peak incidence during the third to fourth decades of life (1, 3). Numerous risk factors have been identified in the pathogenesis of Aspergillus endocarditis. Previous valvular surgery is the most important risk factor, and was reported in 40% to 50% of patients diagnosed with Aspergillus endocarditis (1, 2).
Aspergillus endocarditis of native valves is rare and experience in diagnosis and treatment is limited (1, 4). Only 28 cases of Aspergillus endocarditis were found in a MEDLINE search from 1995 to 2006, and the mortality rate was reported to be higher than 90% despite aggressive surgical and anti-fungal therapies (1). In most cases, predisposing factors were found including underlying cardiac conditions, prosthetic cardiac devices, central venous catheters, and previous antibiotic treatment. In 3.4% of cases with fungal endocarditis, no predisposing factor was reported (1). In this case, the patient underwent pericardiocentesis for pericardial effusion, but we could not find any predisposing factors.
Because of the ubiquitous nature of the organism, establishing a definitive diagnosis of disease caused by Aspergillus is difficult (5). The Aspergillus species is very rarely isolated from blood culture. Many cases are diagnosed on surgical specimens or at autopsy. Recently, antigen detection methods and the polymerase chain reaction have been developed to improve the diagnosis of invasive Aspergillosis (6). Echocardiography is a very important diagnostic modality for Aspergillus endocarditis. The vegetations in Aspergillus endocarditis are large and highly mobile and peripheral embolization is common in early stage disease (1). In this case, the patient presented with iliac artery occlusions and with large mobile vegetations of the mitral valve.
The optimum therapy in patients with Aspergillus endocarditis remains unclear. In general, the largest databases for Aspergillosis treatment include amphotericin B and various surgical modalities (5). In this case, we used a combination of amphotericin B, itraconazole and aggressive surgical treatment, but severe disseminated fungemia reappeared unexpectedly during the early postoperative period with a SMA aneurysm and peripheral artery embolic occlusions. These complications may have been due to delay of antifungal treatment after surgery and dissemination by cardiopulmonary bypass before antifungal therapy was started. Relapsing fungal endocarditis is a complication seen in as many as 30 to 40% of patients who have fungal endocarditis and who survive to complete short-term therapy (7). Thus, all patients who survive long enough to complete acute treatment are potential candidates for long-term suppressive antifungal therapy (1, 3, 8).
Aspergillus endocarditis is rare and there is limited experience with its diagnosis and treatment. Native valve Aspergillus endocarditis is uniformly fatal without immediate and extensive surgical intervention combined with prolonged antifungal therapy.

 XML Download
XML Download