

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Renal transplantation is a widely accepted treatment approach for an increasing number of patients with end-stage renal disease. Because of the improvement in immunosuppressive therapy and management of patients after renal transplantation, long-term patient and renal allograft survival has improved. With the long-term renal allograft and patient survival, some patients develop secondary complications of systemic atherosclerosis, such as aortic aneurysmal or occlusive disease, necessitating operative intervention. In fact, many of these patients are at risk for accelerated atherogenesis due to their long-standing hypertension, uremia and other comorbid factors.
In renal allograft recipients, an abdominal aortic aneurysm (AAA) requiring surgical management may represent a truly life-threatening condition, and a more complicated repair. Aortic reconstruction with aortic cross-clamping places the renal allograft in the pelvis at risk for ischemic damage. To minimize this risk, several different operative strategies have been reported (1-8). We herein report our experience using a temporary shunt for AAA repair in a patient with a renal allograft.
CASE REPORT
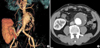
A 40-yr-old man developed end-stage renal disease secondary to chronic glomerulonephritis that had been diagnosed 18 yr before. Thirteen years previously, he had undergone a living-related renal transplantation to the right iliac fossa without complications. The patient was maintained on prednisone and other immunosuppressants such as cyclosporine and mycophenolate mofetil. The transplanted kidney showed excellent function until the diagnosis of AAA. The serum creatinine level was within normal limits during the follow-up period. An abdominal ultrasound for the regular follow-up evaluation was performed in December 2005. The scan revealed an AAA, and subsequent computed tomography (CT) angiography showed an infrarenal AAA measuring 6.4 cm in diameter (Fig. 1). There was no radiographic evidence of leak or rupture.
On preoperative evaluations, myocardial perfusion imaging at rest and under stress revealed an abnormal irreversible perfusion defect in the inferior and basal lateral wall. Coronary angiography showed a focal severe stenosis of the proximal left circumflex coronary artery. However, attempts to pass a balloon failed and he was maintained with medical treatment.
After one month of medical management, he underwent an AAA repair with a tube prosthesis and a temporary aortofemoral shunt. Through a transperitoneal approach, the aorta was dissected up to the renal artery without renal vein division. A separate right groin incision was made to expose the common femoral artery. Because the proximal neck of his AAA was enough to place the temporary shunt, cannulation for a temporary shunt was performed at the level of the perirenal aorta; this shunt was placed in the common femoral artery (Fig. 2). A 16-Fr and a 12-Fr aortic perfusion cannula (Edwards Lifesciences, Irvine, CA, U.S.A.) were used for the temporary shunt, and these two cannulas were connected with a 3/8" connector. After confirming this temporary shunt's function, we performed infrarenal aortic cross-clamping. The total aortic cross-clamping time was 34 min and the renal allograft produced urine throughout the AAA repair with a 16-mm Dacron tube graft. The aortic and femoral cannulation sites were simply closed with previously placed purse-string sutures. The patient recovered without any complications, and the immediate postoperative serum creatinine level was 1.1 mg/dL. During the admission, his serum creatinine level remained within normal limits. He was discharged after a 14-day hospitalization, and subsequent CT angiographic images showed a well-functioning aortic graft with a renal allograft (Fig. 3). His renal function has remained stable over 18 months of follow-up.
DISCUSSION
The long-term patient and renal allograft survival rates after renal transplantation have increased. As a result, the number of patients requiring aortoiliac reconstructive surgery after renal allograft is also increasing. Because patients with functioning renal allografts have a high incidence of concurrent cardiovascular disease, especially hypertension, they may be more susceptible to the development of aneurysmal disease (2, 10). It was recently reported that aortic aneurysms in renal transplant patients have aggressive natural history with high expansion and rupture rates (9, 10). Therefore, one study recommended yearly ultrasounds for the screening of AAA in renal transplant recipients as part of the routine post-transplantation follow-up (10).
Given the solitary arterial supply and lack of collateral circulation of the renal allografts, these allografts are more susceptible to ischemic injury than are the native kidneys. In general, a renal ischemic time of 60 min is safe; this is supported experimentally (11, 12) and in clinical studies (13, 14). Wahlberg et al. (15) emphasized that the most important risk factor for allograft ischemic damage is the clamping time of the aorta proximal to the renal artery; they concluded that aortic clamping above the renal arteries for up to 50 min appears to be safe. In addition, renal function prior to surgery and hypotension during the operation influence ischemic damage.
Although there is no clear evidence that the renal allograft may be seriously damaged by ischemia during aneurysm repair, the risk of ischemic is a concern based on anatomical considerations. Methods have been proposed with the unifying purpose of allowing effective aortic replacement while minimizing the risk of allograft loss. These include the use of temporary shunts (1, 2), extracorporeal bypass (3), cold renal perfusion (4, 5), and general hypothermia (6). However, there are also some reports of successful aneurysm repair without any adjunctive renal protective measures (16, 17). The most obvious method of protecting a renal allograft from an ischemic insult is to maintain perfusion during the aneurysm repair. The use of temporary shunting techniques, as described above, provides native, oxygenated, pulsatile blood flow to the transplanted kidney. In our case, there was a sufficient aortic neck to allow the placement of a purse-string suture and a cannula, so we selected a temporary aortofemoral shunt to avoid renal ischemia. The renal allograft produced urine throughout the AAA repair and there was no transient rise in the serum creatinine level. In addition, we could not identify any deleterious effects from the maneuvers detailed above.
Recently, with the development of endovascular techniques, aortic aneurysms can be repaired without aortic cross-clamping and the associated risk of distal ischemia (7, 8). Endovascular repair may be a new renal protective measure, as the allograft ischemia is limited to the brief time that the graft is ballooned into place. Although the possible disadvantages of endovascular repair with a pelvic renal allograft include emboli to the kidney from dislodged atherosclerotic debris during the procedure, as well as the risk of contrast-induced nephropathy, it may be a safe and effective method for the repair of AAAs in selected patients.
In summary, our case with a temporary aortofemoral shunt technique illustrates the feasibility of avoiding renal ischemia in patients with a renal allograft during AAA repair. This approach can be used in similar patients to prevent jeopardizing the function of a previously placed renal allograft, especially in patients with marginal renal function.


 XML Download
XML Download