

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Most tumors in lower female genital area are originated from vaginal or urethral mucosa (1, 2). Mostly, they are accompanied by apparent symptoms, such as vaginal bleeding or hematuria, which lead to an easy detection of the tumor (2). However, the mass developed at urethrovaginal septum without definite involvement of mucosa of urethra or vagina is rare and it does not show any obvious symptoms or signs except urinary retention (3).
We report a case of endometrioid adenocarcinoma at urethrovaginal septum. The difficulty in diagnosis of the tumor at urethrovaginal septum is discussed.
CASE REPORT
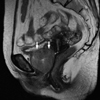
A 61-yr-old woman presented with recurrent urinary tract infection. She had been treated with antibiotics for urinary tract infection several times. She had a history of smoking 1 pack per day for 20 yr, drinking 10 cups of coffee per day for 30 yr. Exposure to diethylstilbestrol during her fetal period was uncertain. She had been receiving hormone replacement treatment with estrogen and progesterone for past 5 yr in a local clinic to alleviate menopausal symptoms including senile vaginitis. The uterus was mobile and non-tender. And the symphysis pubis had been felt as prominent. The mass was enlarged to the size of walnut 4 month later. A pinpoint sized ulceration at lower 1/3 of anterior vaginal wall elevation was noticed after rotating vaginal speculum about 90° to show the anterior vaginal wall. Punch biopsy was performed and the microscopy of the mass revealed endometrioid adenocarcinoma. A magnetic resonance imaging revealed 4.3×4.2 cm sized mass between urethra and vagina (Fig. 1). A positron emission tomography-computed tomography revealed a focal hypermetabolism at the site of mass.
All the results of complete blood count and blood chemistry were within normal limits with exception of urine analysis showing white blood cell and red blood cell count higher than 100/HPF. All serum tumor markers such as CA 125, CA 72-4, CA 15-3, CA 19-9, TA-4, carcino embryonic antigen, and neuron specific endolase were within normal limits. A Pap smear result was normal and no high-risk human papilloma virus was detected.
Anterior pelvic exenteration, bilateral salpingooophorectomy, pelvic lymph node dissection, and urostomy with ileal conduit were performed. An operative finding revealed a walnut sized, soft, well-demarcated mass at urethrovaginal septum. The uterus, both adnexae, and pelvic lymph nodes had normal gross findings. There was no residual disease in the abdomen and pelvis cavity at the completion of the operation. The postoperative course was uneventful except for rectocutaneous fistula. She had no evidence of disease for 24 months.
Pathological examination
Grossly 5×2×1.5 cm sized urethrovaginal mass protruding into urethra with focal villous appearance was present. The tumor had formed a fistula tract into the vagina (Fig. 2A) which was replaced by defect of punch biopsy. On serial section, the cut surface of the tumor was largely necrotic. The epicenter of the tumor was between urethra and vagina. Microscopically mucosal invasion was noticed in both vagina and urethra.
Microscopically grade 2 endometrioid adenocarcinoma was confirmed (Fig. 2B). No histological evidence of endometriosis was identified. The endometrium and the myometrium were atrophic. The cervix and both adnexae appeared normal. No lymph node metastasis was seen.
The immnunohistochemical staining was negative for estrogen receptor (ER), progesterone receptor (PR), CD10, hMLH 1, and hMSH 2. But bcl-2 was positive in 30% of tumor cell. And p16 and p53 were positive in 85% and 90% of tumor nucleus, respectively.
DISCUSSION
Primary vaginal cancer constitutes about 2% of malignant neoplasm of the female genital tract (2). Eighty four percent of vaginal cancer was secondary, from the cervix (32%), the endometrium (18%), the colon and rectum (9%), the ovary (6%), or the vulva (6%). Most patients with vaginal cancer experience painless vaginal bleeding and discharge (2). Primary carcinoma of the female urethra is rare malignancy, accounting for less than 0.1% of all female genital malignancies (1). Most tumors involve the anterior or the distal urethra and may be confused with a urethral caruncle or mucosal prolapse. The most common symptoms include urethral bleeding, hematuria, dysuria, urinary obstruction, urinary frequency, and a mass at the introitus (2).
Tumors in lower female genital area were relatively rare but mostly it can be easily detected because of its early appearing symptom when it involves vaginal or urethral mucosa. But, Nagai et al. (3) reported that even 7 cm sized leiomyoma in urethrovaginal septum caused no symptoms except for urinary retention. Recurrent urinary tract infection was the only clue to suggest the mass in urethrovaginal septum for the first time in this case. It is essential to examine anterior vaginal wall in patients with urinary tract symptoms including recurrent urinary tract infection, and urinary retention.
We would like to name the urethrovaginal septum as the "retropubic shadow" for gynecologists for the following reasons. Firstly, fingertips of palpating vagina direct to promontory. It is another direction to urethrovaginal septum. Colpogram of healthy women revealed that the upper third of the vagina lays almost horizontally to the coccyx and vaginal axis formed by levator ani make fingertips entering vaginal cavity to go to bending toward promontory. This is remarkable at pelvic examination, because of more acute vaginal axis with patient's straining of levator ani (Fig. 3A) (4). Secondly, the small mass at urethrovaginal septum could be misunderstood as symphysis pubis (Fig. 3B). Thirdly, the actual primary urethrovaginal carcinoma like in this case is not accompanied by evident symptoms such as hematuria or vaginal bleeding until the tumor penetrates the mucosa of vagina or urethra (5). Lastly, the rarity of this condition makes it hard for physicians to consider the possibility of this particular disease (2).
Extraovarian endometrioid adenocarcinoma and adenosarcoma could be developed from endometriosis with unopposed estrogen replacement (5-8). However, in this case, the woman had been received estrogen with progesterone and immunohistochemical staining was negative for ER and PR. And endometriosis as precursor lesion was not identified. So, we think that the tumor in this patient have different pathogenesis compared to previously reported cases.
To the best of our knowledge, this is the first reported case of extraovarian endometrioid adenocarcinoma developed at urethrovaginal septum. Understanding normal functional anatomy and meticulous physical examination are essential to early detection of this rare tumor in urethrovaginal septum.


 XML Download
XML Download