

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Esophageal pH monitoring was first used by Tuttle and Grossman in 1958 (1). Miller first reported in 1964 the use of an indwelling pH electrode positioned above the lower esophageal sphincter (LES) to continuously monitor the intraesophageal pH (2). This technique overcame many of the weak points of the other tests that had been used to detect gastroesophageal reflux.
Ambulatory 24-hr esophageal pH monitoring is increasing in popularity as the standard method for measuring esophageal exposure to gastric acid. It provides quantitative data on esophageal acid exposure as well as the temporal correlation between symptoms and actual acid reflux events. Since acid reflux into the esophagus is a physiological event even in normal subjects, discrimination between physiological and pathological reflux is often difficult (3). Good temporal correlation between a distinct pathological event such as chest pain and a pH drop on the recording provides evidence of pathogenicity (4). However, if any symptomatic correlation is not present, then only the quantifiable parameters can be used to determine the presence of any abnormality. As this technique has become widely available, questions have been raised regarding the best parameter to use to measure esophageal acid exposure, the optimal thresholds to differentiate normal from abnormal and the influence of gender and age on the measurement (5-8).
Most studies concerned with the standard values of esophageal pH monitoring have been done in Western countries (5, 6, 8-10). Because the genetic and environmental factors are different between Western and Eastern countries, there might also be a difference in the degree of gastroesophageal reflux between them. Actually, the reported pH standards have shown a considerable variability between Western countries and even among regions of the same country (6, 7, 10, 11). Establishing the normal values of esophageal pH monitoring for Eastern countries different in many aspects from Western countries would be of great benefit for better understanding of gastroesophageal reflux disease (GERD) and its proper treatment. There have been a few previous reports about the normal reflux parameters in Eastern countries such as China (12, 13). Therefore, the aim of this study was to establish the normal values for gastroesophageal acid exposure in healthy Koreans.
MATERIALS AND METHODS
Subjects
This study was performed at 7 university hospitals in Korea from May to October 2007. Each volunteer was carefully interviewed and when appropriate, he or she underwent a physical examination and laboratory studies to exclude systemic disorders that might alter esophageal motility or predispose to GERD. Volunteers were excluded if there was any history of heartburn, regurgitation, chest pain, dysphagia for solids or liquids, odynophagia or use of antacids, promotility drugs, histamine-2 receptor blockers or proton pump inhibitors. Additionally, none of the volunteers had a history of esophageal or gastric surgery, diabetes mellitus, alcoholism, neurological disorders or collagen vascular disorders. The medication histories were closely reviewed and none of the volunteers were taking any drugs that would influence acid secretion or esophageal function at the time of the study. Upper endoscopy was performed on all the volunteers to exclude hiatal hernia, reflux esophagitis or other organic diseases such as peptic ulcer. Informed written consent was obtained from each subject prior to the study and this study was approved by the Institutional Review Board at each university hospital.
Ambulatory 24-hr esophageal pH monitoring
Ambulatory 24-hr esophageal pH monitoring was performed immediately after standard esophageal manometry with using a single-use monocrystalline antimony pH probe (Zinetics 24, Medtronic Inc., Minneapolis, MN, U.S.A.). A cutaneous reference electrode placed on the upper chest was also used. All the electrodes were initially calibrated in buffer solution of pH 7 and then in buffer solution of pH 1. The pH catheter was introduced transnasally into the stomach and then it was withdrawn back into the esophagus until the electrode was 5 cm above the proximal margin of the LES. The subjects were encouraged to eat regular meals with restrictions for the intake of drink or food with a pH below 4. All the subjects recorded their meal times (start and end), body position (supine and upright) and any symptoms in a diary. The data were collected using a portable data logger (Digitrapper Mark III, Synetics Medical Co., Stockholm, Sweden) with a sampling rate of 4 sec, and the data was then transferred to a computer for analysis with using Polygram for Windows® (Release 2.04, Synetics Medical Co.). A decrease in pH below 4, which was not induced by eating or drinking, was considered the beginning of a reflux episode, and the following rise to pH above 4 was considered to be the end of such an episode.
All the tracings were inspected by one of the authors to confirm the computerized calculations and to assure the quality of the recordings. The six parameters assessed for gastroesophageal reflux were the total percentage of time the pH was <4, the percentage of time the pH was <4 in the supine and upright positions, the number of episodes the pH was <4, the number of episodes the pH was <4 for ≥5 min, the duration of the longest episode the pH was <4 and the composite score (14). To obtain the composite score, a scoring system based on the standard deviation of the mean of each of the six components was used (5, 10). The simplified formula for scoring each of the six components is:
Component score = (Patient value-mean / Standard deviation) + 1
Statistical analysis
The data were expressed as median values (range) unless otherwise noted. The normal values for each parameter were assessed by calculating the 95th percentile for the subject group. The age of 40 was used to dichotomize the subject sample because visual inspection of the data suggested it would maximize the probability of finding an age effect on the pH variables. The Mann-Whitney test and the Kruskal-Wallis test were used to assess the effect of age and gender on each esophageal pH parameter. A p<0.05 was considered statistically significant. Statistical calculations were performed using the SPSS version 10.0 for Windows software (SPSS Inc., Chicago, IL, U.S.A.).
RESULTS
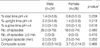
Fifty healthy volunteers (24 males and 26 females; mean age, 45 yr; range, 19-66 yr) were recruited for this study. Table 1 summarized the demographic data of the 50 volunteers who constituted the study population. The values for the composite score and the six parameters used to express the esophageal acid exposure in the 50 healthy volunteers are shown in Table 2. The median and 95th percentile values for the percent time pH <4 for the total monitoring period and the composite score were 1.1, 4.3, 4.7, and 14.2, respectively. There was no difference in all the pH parameters between male volunteers and female volunteers (Table 3). In addition, there was no difference in all the pH parameters between young volunteers and old volunteers (Table 4). The interaction of gender and age did not show any significant difference for all the pH parameters (Table 5).
DISCUSSION
We have demonstrated that physiologic gastroesophageal reflux occurs in healthy adults. The results of our multicenter study for the amount of physiologic gastroesophageal acid reflux in 50 healthy Koreans can be summarized as follows: 1) gender does not independently influence the pH parameters; and 2) age also does not influence the pH parameters.
Men are generally known to secrete more gastric acid than women and this is explained in part by the larger body mass of men (15, 16). In a previous report, male volunteers showed higher median values than women volunteers for all the pH parameters except for the percentage time pH <4 in the supine position (6). In another report, there was no difference in esophageal acid exposure between males and females when the results of 24-hr pH monitoring were expressed as the composite score (5). They suggested that using the composite score to determine when a patient had increased esophageal exposure to gastric juice could eliminate the necessity of having separate normal values for men and women. In present study, there was no difference in all the pH parameters between males and females. In one previous prospective study about acid output, gender had no significant effect on the basal output of acid and it had only borderline significant effects on the peak acid output (17). This fact could explain our results, even though differences of genetic and environmental factors between Koreans and Western populations do exist.
In the present study, there was no reliable association between the esophageal pH parameters and age. Schlesinger et al. first raised the possibility that increasing age had an effect on the esophageal pH parameters (7). It was also reported that older subjects showed significantly higher values for the total and upright percentage of time of pH <4 as well as the total number of reflux episodes >5 min (18). But in that study, the sample size was relatively small and older controls were obtained from a hospitalized veteran population, and this veteran population had a high prevalence of hypertension and diabetes mellitus. On the other hand, the results of a large population study on 110 healthy subjects did not show an independent effect of age on the pH parameters (6). This result was similar to our result. Thus, for clinical purposes, it seems that age generally does not have an important effect on the physiologic parameters of acid reflux.
The normal esophageal pH standards developed in the present study have some merits. First, in our study, all the healthy volunteers underwent upper endoscopy to exclude asymptomatic esophagitis and hiatal hernia. In two large Western studies concerned with the normal ambulatory esophageal pH values (5, 6), they did not perform endoscopy. Therefore, they could not exclude the subjects with asymptomatic esophagitis or hiatal hernia. In the present study, we excluded these subjects by performing endoscopy. Second, the distribution of gender and age of the healthy volunteers in our study was uniform (data not shown).
Nevertheless, our study still had some limitations. First, the number of subjects in this study was not large; this could raise the possibility of a type-2 error. However, to be included in the study, the volunteers were required not to have any clinical evidence of GERD and they were also without endoscopic documentation of reflux esophagitis and hiatal hernia. These facts reduced the number of subjects for the study, so as to render our healthy volunteers as being appropriate. Second, although our study population was carefully screened to be healthy and asymptomatic and we excluded the subjects who had reflux esophagitis or hiatal hernia, many of the subjects might have H. pylori infection with or without chronic atrophic gastritis. There is a higher prevalence of H. pylori infection in Koreans than in Western populations (19). Mild H. pylori-associated chronic active superficial gastritis had little effect on gastric acid output, whereas severe chronic active gastritis was associated with a lower gastric acid output (17). This fact could also explain the lower values of the reflux parameters in our study as compared to the Western studies. Finally, because this study was performed at 7 medical centers, there would be bias of the reflux parameters among each center. To lessen the bias, we defined a standard method of ambulatory 24-hr esophageal pH monitoring and then we started this study. In addition, the coefficient of variation for the reflux parameters among each center was less than 40%, except the percentage of time the pH was <4 in the supine positions.
The normal values of the pH parameters, as 95th percentiles in 3 previous Western studies (5, 6, 10) and in our study, are shown in Table 6. Almost all the parameters except the number of reflux episodes were lower in our study than those in the Western studies. Many factors, including the differences in the age distribution of the control subjects, the real population differences for gastroesophageal reflux and the different incidence of H. pylori infection, could have contributed to these results.
In conclusion, our multi-center data were based on 50 healthy volunteers, and these data provides the normal values for esophageal pH monitoring in Koreans. It could allow for greater confidence in identifying those patients with GERD. However, no database is perfect because of the well-known variability of acid exposure from day to day and the inherent problems with the pH probe (i.e., it may get buried in the esophageal mucosa and so miss reflux episodes) (8, 20). On the basis of our results, these normal esophageal pH values can provide reference data for future clinical and research studies in Korea.





 XML Download
XML Download