

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Herpes zoster is a localized disease characterized by unilateral radicular pain and a vesicular eruption caused by the varicella zoster virus. In addition to sensory neurons, it may also affect motor neurons in rare cases. Herpes zoster ophthalmicus has caused extraocular muscle palsies of the third, fourth, and sixth cranial nerves in 7 to 31% of patients (1-3). The third nerve appears to be the most commonly affected, and the fourth nerve, the least. In herpes zoster ophthalmicus, extraocular muscle palsies usually appear 2 to 4 weeks after a rash, but sometimes occurs simultaneously with a rash or more than 4 weeks later. The extraocular muscle palsies associated with herpes zoster ophthalmicus is a transient, self-limited condition, usually seen in the elderly (4, 5). Such cases have not often been reported, although extraocular muscle palsies caused by herpes zoster ophthalmicus appears frequently.
CASE REPORT
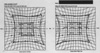
An 80-yr-old female had been in good health until she developed sharp, lancinating pain over the left side of the scalp. Four days later, a vesicular eruption occurred in the distribution of the ophthalmic division of the trigeminal nerve on the left side of the scalp, and this was accompanied by diplopia (Fig. 1). On ophthalmologic consultation, diplopia was present in the primary position and was more pronounced on attempted abduction of the left eye (Fig. 2A). A Hess chart shows the ocular movements of left VI nerve palsy in this case (Fig. 3). The remainder of the physical examination was within normal limits. Blood tests were normal, including liver and renal function tests, whereas the white blood cells (WBCs) were increased at 11,500 per mL, with 82.4% being segmented neutrophils. The patient suffered from fever and headache, and thus the cerebrospinal fluid (CSF) was examined to rule out herpes zoster encephalomeningitis, which revealed that varicella zoster virus IgG and IgM were elevated. However, other CSF findings such as WBC counts, proportions of lymphocytes, and the protein level were within normal limits. There were no specific findings on the neurological examination. Brain magnetic resonance imaging was normal except for old infarctions in both basal ganglia and the periventricular white matter. The good general health and negative neurologic and laboratory examinations in our patient excluded other causes of acquired paresis of the nerve, such as vascular cerebral accidents, brain tumors, and encephalitis. A diagnosis of herpes zoster was made, and acyclovir 800 mg was given intravenously for 5 days. Despite our advice to continue therapy, the patient wanted to discharge after 5 days. So further treatment was stopped. The skin lesions resolved within 1 week, although the diplopia was still present. On follow-up examination 7 weeks later, the abducens nerve palsy had improved without extra treatment (Fig. 2B).
DISCUSSION
Sixth nerve palsy is the most common cranial nerve palsy affecting the ocular motility. Patients present with horizontal diplopia, which is worse on looking to the affected side, and often the face turns to the affected side.
The third, fourth, and sixth cranial nerves control eye movements. The third nerve, which controls internal, inferolateral, superolateral, and superomedial eye movements, is infected most commonly with herpes zoster, whereas abducens palsy complicating herpes zoster is relatively uncommon (6-8).
The mechanism through which the ocular motor nerves or muscles are involved in zoster is not clear. Denny-Brown et al. (9) found that motor neuritis was independent of the inflammation of any ganglion. Edgerton (2) and Godtfredsen (10) postulated that the involvement of the second, third, fourth, and sixth nerves was attributable to contiguous intracavernous radiculomeningitis. While contiguous intracavernous spread is a distinct possibility, Sunderland and Hughes (11) concluded that there was no communication between the fifth nerve and the third, fourth, and sixth cranial nerves, although sympathetic branches temporarily attached to the abducens nerve as they passed from the carotid plexus to the ophthalmic and maxillary nerves. Kreibig (12) postulated that the extraocular palsies were due to perivasculitis-myositis, rather than to a neural origin. Muscle ischemia remains a strong possibility, as does a combination of orbital nerve and muscle inflammation. Therefore, isolated abducens nerve palsy might be caused by circumscribed orbital myositis or a lymphocytic cranial motor neuropathy.
Multiple mechanisms have been documented in the cases examined histopathologically, and the histology of the lesion within one patient may have a variety of forms in different locations (13). It is probable that all of these mechanisms of disease, working separately or simultaneously, are responsible for the clinical presentation (14).
There are different suggestions about the treatment of the paralytic lesions that complicate herpes zoster. Some authors have examined the effectiveness of antiviral therapy and adrenal cortex hormones. As the paralytic lesions tend to resolve spontaneously, the effects of specific treatment are unclear (15, 17). In our case, the paralytic lesion resolved completely within 7 weeks without specific treatment. The recovery time was similar to that in the previous report, the 6 and 8 weeks respectively (7, 8). The prognosis for spontaneous recovery of extraocular muscle function has been reported to be favorvable (4, 16).


 XML Download
XML Download