

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Uterus didelphys with obstructed hemivagina is an obstructive Mullerian anomaly caused by lateral nonfusion of the Mullerian ducts with asymmetric obstruction (1). This condition is almost always associated with renal agenesis ipsilateral to the obstruction, which could be due to embryologic arrest at gestation week 8 that simultaneously affects the Müllerian and metanephric ducts (1). However, other accompanying renal anomalies, such as, renal dysplasia, a double collecting system, and ectopic ureter are possible, although only a limited number of such cases have been reported (2, 3).
Various clinical symptoms, such as severe dysmenorrhea, lower abdominal pain, paravaginal mass excessive foul mucopurulent discharge, and intermenstrual bleeding, which are dependent on the existence of uterine or vaginal communications, have also been presented (4).
Excision of the vaginal septum is the treatment of choice for a unilateral vaginal obstruction. However, excision of the vaginal septum using scissors and subsequent anastomosis of the vaginal mucosa are often difficult to perform in girls because of small vaginal dimensions and frequently a high septum location compared with the entire vaginal wall. Moreover, hymenectomy must be performed for this intervention.
Instead of the transvaginal resection of vaginal septum, there have been several reports on the procedures using hysteroscopy (5-7). In the present case, hysteroscopic resection of the vaginal septum was performed under transabdominal ultrasound guidance to preserve hymen integrity. Given the limited information available on this topic, the authors describe hysteroscopic resection of the vaginal septum in a girl with uterus didelphys with obstructed hemivagina, for the first time in Korea.
CASE REPORT
A 14-yr-old girl visited the Department of Obstetrics and Gynecology at Seoul National University Hospital because of persistent vaginal spotting following menstruation. She experienced menarche 8 months before admission, and her menstruation cycles were rather regular with a 60-day interval, without pronounced dysmenorrhea.
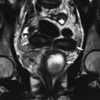
Sonographic examination revealed two distinct uteri and a cystic mass along the left lateral wall of vagina. Magnetic resonance imaging verified the anomaly, i.e., uterus didelphys with obstructed hemivagina and ipsilateral agenesis of the left kidney (Fig. 1).
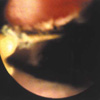
Under general anesthesia, we performed a hysteroscopy without speculum or tenaculum. For endoscopy, a 3.5-mm minihysteroscope (Versascope, Gynecare, Ethicon, Sommerville, NJ, U.S.A.) was used to preserve the integrity of the hymen; saline was used as a distending medium. Because of the large bulging mass, vaginal space appeared narrowed. An endoscopic vaginal exploration showed the presence of a right uterine cervix at the 2 o'clock position. An abdominal ultrasound examination was performed to confirm the minihysteroscope location. The obstructed vaginal septum and the minihysteroscope tip were discriminated from the fluid-filled vagina. To confirm the bladder position and to avoid bladder injury, the bladder was filled with saline after inserting a 16F Foley catheter. The vaginal septum was punctured at a site approximately 2.0 cm lower from the right uterine cervix with the minihysteroscope under transabdominal ultrasound guidance (Fig. 2). A moderate amount of pus-like material was drained from the punctured vaginal septum. Subsequently, without disrupting the hymen, a 8.7-mm resectoscope (Karl Storz, Tuttlingen, Germany) was inserted into the vagina, and an electrolyte-free 5:1 sorbitol/mannitol solution (Urosol, CJ, Korea) was used as the distending medium (Fig. 3). Through the punctured site, we dissected the vaginal septum using a cutting electrode point until the diameter of the opening reached about 4 cm (Fig. 4). After vaginal septum dissection, the vaginal space had become enlarged and the left cervix was clearly visible. The operation took about 20 min to perform. Intervention was simple and completely bloodless. At the 6-month follow-up the patient was totally symptom-free.
DISCUSSION
Uterus didelphys with an obstructed hemivagina usually requires surgical treatment for the resolution of clinical symptoms. The traditional surgical method requires transvaginal resection of the obstructed septum, and this continues to be the most widely used modality. However, conventional excision of the vaginal septum performed with scissors requires hymenal disruption and wide exposure of the vagina. In addition, the procedure presents technical difficulties because edges must be sutured in a limited surgical field (8).
Hysteroscopic resection of an obstructed septum, as described in the present case, is simple and fast, and does not require any specialized surgical technique. Moreover, this modality preseves the hymen integrity, and thus should be considered for young women. Moreover, hysteroscopy provides near ideal conditions for intervention as it considerably enlarges the surgical view. In addition, transabdominal ultrasound guidance improves interventional accuracy.
According to our experiences of transvaginal resection of an obstructed septum in such cases, the method is performed easily only in cases with large hematocolpos. A relatively small hematocolpos presents greater difficulties in terms of deciding upon the resection site. However, hysteroscopic resection of the vaginal septum under transabdominal ultrasound guidance facilitates easy correction of small hematocolpos.
In the present case, clinical symptoms resolved completely after vaginal septum excision at the 6-month follow-up, though we consider that a longer follow-up is necessary due to the possibility of recurrence, and suggest that outpatient hysteroscopy is appropriate for monitoring recurrence. In a more general sense, systematic comparative studies are required on the effectiveness of hysteroscopic intervention versus conventional transvaginal resection.
In conclusion, hysteroscopic resection of the vaginal septum under transabdominal ultrasound guidance in cases of uterus didelphys with an obstructed hemivagina was found to provide an excellent alternative to conventional treatment. Therefore, we report this case with the discussion on the advantages of hysteroscopic resection of vaginal septum over the conventional treatment.


 XML Download
XML Download