

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Transfusion-associated primary cytomegalovirus (CMV) disease is known to cause significant morbidity and mortality among premature infants born with birth weights less than 1.5 kg (very low birth weight infants, VLBWI) (1). CMV transmission via blood transfusion can best be prevented by using only blood products from CMV seronegative donors. However, the prevalence of CMV seropositivity among blood donors limits the availability of seronegative blood products in hyperendemic area such as Korea, where donor blood is not routinely screened for CMV antibodies. To date, few studies have examined the incidence of CMV infection acquisition through transfusion in VLBWI in endemic areas. Without knowledge of this incidence, there is little information available for determining best transfusion practices for reduction of transfusion-acquired CMV infection in endemic areas. As a result, standardization of transfusion policies in Korean hospitals is lacking. We sought to investigate the incidence of acquired CMV infection in a hyperendemic area when VLBWI were given CMV IgG-positive blood. We compared the incidence and characterization of VLBWI who acquired CMV infection when using filtered-irradiated versus nonfiltered-nonirradiated blood, and examined the time required for VLBWI to clear passively-derived anti-CMV IgG.
MATERIALS AND METHODS
Subjects
We compared the incidence of acquired CMV in two neonatal intensive care units (NICUs) with different transfusion practices. We enrolled all VLBWI admitted to the NICU of hospital A between 1 February 2000 and 30 June 2001 and all VLBWI admitted to NICU of hospital B during the same time period, who required either packed RBC (PRBC) or platelet transfusions.
In hospital A, the routine procedure was to transfuse blood products that had been filtered through RCXL™ (Pall Biomedical, Inc., East Hills, NY, U.S.A.) for PRBC and PXL™8 (Pall Biomedical Inc.) for platelets. In hospital B, the routine policy was to use nonfiltered-nonirradiated blood products. VLBWI from either hospital were excluded from the analysis if: 1) they had congenital CMV infection as evidenced by positive urine CMV culture within 2 weeks of life, 2) outpatient department (OPD) follow-up was not possible, as study subjects were followed until CMV seronegativity was documented, 3) they expired during study period, or 4) parents did not consent.
The guidelines for PRBC (2) and platelet (3) transfusions were followed strictly at both hospitals. In each instance, the volume of blood given per transfusion was 10-15 mL/kg. Some VLBWI from both hospitals were fed their own mother's expressed breast milk, which had been frozen at -20℃ for 4-10 days and thawed just prior to each feeding. None were fed fresh maternal or fresh banked breast milk and breast milk given in both hospitals were not evaluated by CMV culture/PCR for infectivity. Parental consents were obtained prior to enrolling subjects. This study was approved by the institutional review board of the Asan Medical Center and Samsung Cheil Hospital.
Tests on transfused blood and VLBWI
Aliquots of all transfused PRBC anticoagulated with CPD solutions and platelet concentrates provided to hospitals A and B by the Korean Red Cross were tested for total CMV IgG and IgM by enzyme linked fluorescent assay (VIDAS CMV IgG, IgM, bioMerieux, Marcy-l'Etoile/France). All blood donors were screened for hepatitis B, C, HIV, Treponema pallidum, and liver function tests, to exclude other infection. In hospital A, PRBC units were divided into three bags by an aseptic technique (last bag to be used within 14 days of preparation), limiting patient-donor exposures. In these cases, one bag per donor was tested for CMV IgG and IgM.
All RBC products and platelet concentrates, usually 8-11 days and 4-5 days old after donation, respectively, were irradiated at 25 Gy for 179 sec (CIS biointernational, Filiale de Compagnie ORIS Industrie S.A., France) prior to transfusion to prevent postransfusion graft-versus-host disease. The instrument was dosimetrically checked (International Specialty Products, RAD-SURE™, Wayne, NJ, U.S.A.). At hospital B, transfused blood products of 3-5 days and 2-3 days old PRBC and platelets, respectively, were not filtered nor irradiated prior to transfusion. All subjects were tested for CMV IgG and IgM (VIDAS CMV IgG, IgM, bioMerieux, Marcy-l'Etoile/France) at birth and every 3-4 weeks until the infants became seronegative.
Diagnosis of CMV infection
Diagnosis of acquired CMV infection was ascertained by negative urine CMV culture at birth and positive urine CMV culture thereafter, and by CMV IgM seroconversion. Clean voided urine specimens were collected via urine bag at birth and every 3-4 weeks until 12 weeks after the final transfusion. For those who did not receive transfusion in hospital A, CMV urine cultures were obtained every 5-6 weeks during hospitalization and monthly after discharge. To ensure viral viability and prevent bacterial overgrowth, all urine specimens were stored at 4℃, and packed in wet ice for transport.
Isolation of CMV
Urine supernatant samples (0.5 mL) were pipetted into tissue culture tubes containing MRC-5 cell sheets (ATCC CCL-171) that had been incubated for 3 days in MEM medium (Gibco/BRL, Rockville, MD, U.S.A.) supplemented with 10% newborn calf serum, 100 unit/ml penicillin and 100 µg/mL streptomycin. Each culture tube was then centrifuged at 1,700 rpm for 40 min at room temperature to allow the virus to adsorb onto the cell sheet, treated with MEM medium containing 5% newborn calf serum, and incubated at 35-36℃ for 1 day. IFA with specific antibodies (DAKO, m#0854, Denmark) was then carried out on the monolayers. CMV AD169 (ATCC VR-538) and MRC-5 tissue culture tubes with or without viral inoculation were used as the positive and negative controls, respectively.
Statistical analysis
Statistical analyses were performed using SPSS 10 for Windows (SPSS, Inc., Chicago, IL, U.S.A.); p<0.05 was considered statistically significant. Means with standard deviations are given, and Student t-test, Mann-Whitney test, chi-square and Fisher's exact tests were used where appropriate. For evaluating the relationship between gestational age and level of serum CMV IgG, linear regression analysis was used. To test the difference of rate of decline of serum CMV IgG from birth between transfused and nontransfused groups, summary statistic approach and Student t-test were used.
RESULTS
Of 112 eligible VLBWI from hospital A, 1 singleton with congenital CMV infection and 5 VLBWI whose parents refused to consent were excluded, resulting in recruitment of 106 (80 transfused and 26 nontransfused) VLBWI from hospital A. The parents of all 20 VLBWI eligible for the study from hospital B provided consent. All infants, including 9 sets of twins, were followed for the full study period; none were lost for follow-up.
The patient characteristics for the transfused VLBWI are shown in Table 1. The VLBWI who received filtered-irradiated blood products had more transfusions overall, but the number of donor exposures was similar between the two groups. The numbers of VLBWI fed frozen breast milk were similar in both groups. None of study patients received breast milk after discharge due to lack of its availability except one patient in filtered-irradiated blood group who was seronegative at birth and never acquired CMV despite of 2 months period of frozen breast milk feedings. A few infants from hospital A received other blood products: 4 received albumin, 4 intravenous IgG, and 9 were treated with fresh frozen plasma (FFP). None of the infants in the nonfiltered-nonirradiated blood group received other products.
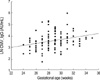
The overall incidence of CMV IgG seropositivity in the enrolled VLBWI at birth was 121/126 (96%). The CMV IgG titer correlated with gestational age at birth (Fig. 1): Linear regression analysis: Ln(IgG)= 0.8410 (s.e:0.8433)+0.0969 (s.e:0.0293)×gestational age (weeks). The percentages of CMV IgG positivity of the filtered-irradiated and nonfiltered-nonirradiated blood products were 96% and 93%, respectively. The CMV IgM was positive only in cases of acquired infection observed after transfusion.
The overall incidence of acquired CMV infection among transfused VLBWI was 4/100 (4%): 2/80 (2.5%) for filtered-irradiated blood and 2/20 (10%) for nonfiltered-nonirradiated blood (p>0.05). All positive urine CMV cultures occurred during hospitalization and CMV infection was only observed among the transfused group in hospital A: None of the 26 nontransfused VLBWI in hospital A showed positive urine CMV culture nor CMV IgM at mean age of 157 days. None of the 4 transfused VLBWI who were seronegative at birth acquired CMV infection, despite multiple transfusions (range: 4-11 times). Of them, 3 received filtered-irradiated blood products from seropositive donors and 1 received nonfiltered-nonirradiated blood products from seropositive donors.
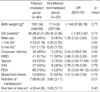
The clinical characteristics and outcomes of the 4 VLBWI who acquired CMV infection are shown in Table 2. Only one VLBWI of the nonfiltered-nonirradiated group was fed frozen breast milk, receiving it for the first 29 days combined with formula. 3 of 4 VLBWI who acquired CMV had detectable serum CMV antibody titers, but low (8, 8, 14 AU/mL) at the time of their last transfusion. No one received immunoglobulin or albumin.
The rate of decline of passively acquired CMV IgG antibody titers in the 100 transfused infants was not affected by transfusion (p=0.0585) (Fig. 2, 3), but did differ depending upon the initial titer. As little as 1-2 months was required to negatively seroconvert the CMV IgG titer in some cases, but almost all (97.5%) of the infants were CMV antibody-negative by 10 months (mean: 5.5 months, range: 36-387 days) (Fig. 4).
DISCUSSION
Prior to the era of leukoreduction and irradiation, the rate of CMV acquisition among seropositive VLBWI receiving transfusions of fresh, CMV unscreened, nonirradiated, nonfiltered blood from a donor population in which seropositivity varied from 34-45.3% was 0-9% (1, 4, 5) compared with 0-0.8% after transfusion of CMV seronegative blood to CMV seronegative recipients (6, 7). The removal of the vast majority of WBCs from RBCs collected from seropositive donors decreases the transmission of CMV among seronegative recipients (8, 9); it has been reported that approximately 5-10% of original WBCs remained in the RBC components filtered with first-generation filters and this number of WBCs may be sufficient to transmit CMV to the recipients via lymphocyte activation. Some even speculate that irradiation and/or storage of blood from CMV-seronegative donors cannot prevent the reactivation of preexisting CMV in recipients, because non-viable irradiated WBCs retain antigenicity and may trigger the activation of CMV in lymphocytes of infected recipients.
In our study, the rate of CMV infection was 4% among seropositive VLBWI from a blood donor population with 95% CMV seropositivity. The rate of acquired CMV infection was 2/80 (2.5%) in the filtered, irradiated group compared to 2/20 (10%) in the nonfiltered-nonirradiated group (p>0.05), suggesting that filtering or irradiation of CMV seropositive blood products did not seem to significantly reduce transfusion-associated CMV infection among VLBWI in hyperendemic area. The rate of CMV acquisition among seronegative VLBWI was 0% despite of multiple nonfiltered-nonirradiated transfusions with CMV seropositive bloods which may have been related to limited number of seronegative VLBWI. The overall observed power in our sample was only 0.233.
The rate of CMV acquisition among filtered, irradiated group is substantially lower than that of 9% incidence of CMV infection found in a similar study using a donor population with 97-100% CMV seropositivity (10). The difference in the rate of CMV infection when VLBWI were given filtered-irradiated blood in similar hyperendemic areas may arise from differences in the use of breast milk feedings (11, 12). Neither of the 2 VLBWI who acquired CMV in the filtered-irradiated group in our study were fed any breast milk, while almost all of the subjects in the previous study (10) were fed expressed maternal breast milk. We also used blood that had been stored for longer periods, a practice that results in lower transmission rates (13, 14).
It is important to note that in contrast to the serious morbidity related to primary CMV disease reported among seronegative recipients of seropositive blood (15-17), there were no CMV-associated fatalities in our CMV-infected VLBWI or in those reported by Ohto et al. (10). This may suggests that maternally-derived CMV antibodies are capable of modifying the severity of CMV infection (18-20) as reported in acquired CMV infection transmitted via breast milk in endemic area (21, 22). However, this protective mechanism may not last long, as passively transferred CMV IgG eventually decreases. Galea et al. reported that 36 of 38 VLBWI lost their passive CMV antibodies within 10 months (6). Similarly, we found that 97.5% of our VLBWI seroconverted within 9-10 months (mean: 5.5 months, range: 36-387 days), and the rate of CMV antibody loss was not affected by transfusions including FFP (p=0.058). These results strongly support the use of WBC-reduced cellular blood components (or equivalent measures) as infants reach seronegative status. This should reduce transfusion-transmitted CMV infection in the examined hyperendemic areas as those neonates born with CMV seronegativity receiving unscreen or CMV seropositive blood in less endemic area (23, 24). Furthermore, medical staff in hyperendemic areas should plan to monitor CMV IgG levels at regular intervals to detect the turning point of seroconversion.
It has been suggested that the use of γ-irradiation will decreases transfusion-transmitted CMV infection by mounting an immune response via indirect prevention of T-lymphocyte proliferation (25, 26) and the use of γ-irradiated blood products in newborn infants has been strongly suggested (27). We found a CMV infection rate of 2/20 (10%) using relatively fresh nonirradiated-nonfiltered blood in comparison to the previously reported 1/19 (5%) (10) using irradiated-nonfiltered seropositive blood. Infected 1 of 2 VLBWI in our nonirradiated-nonfiltered blood group had been fed with frozen breast milk. Although freezing breast milk is thought to reduce CMV infectivity (28) and nosocomial transmission of CMV may not occur frequently (29), the extent to which this infant was exposed to breast milk and other potential source of nosocomial source is unknown. Based on our findings, further investigation is warranted to delineate the effect of irradiation to reduce CMV infection.
The total volume of transfused blood has been identified as an important risk factor for the development of significant transfusion-transmitted CMV disease. Yeager et al. (4) reported that 24% of infants who were born to seronegative mothers but received more than 50 mL of PRBC from at least one seropositive donor became infected. Consistent with this, the volume of PRBC required for VLBWI who acquired CMV infection in our population of hospital A far exceeded those who did not acquired CMV infection (230 mL/patient vs. 68.9 mL/patient). Beneke et al. reported that higher geometric mean titers of CMV IgG of transfused blood may prevent transmission of CMV (30). In contrast, our study showed that CMV IgG titers of the transfused blood was higher but not statistically significant in infants who acquired CMV infection than those who did not (36.1±27.5 AU/mL vs. 31.6±20.1 AU/mL). The mean CMV IgG titers of the recipients sera were similar between these groups (23.6±11.8 AU/mL vs. 21.6±31.4 AU/mL).
Several limitations of this study include lack of control for nosocomial, environmental infection (breast milk) and the small sample size. For a prospective randomized trial, we would need 177 transfused infants per group assuming a relative risk of 0.25 (or a relative reduction rate of 75% from 0.10 to 0.025), p<0.05, and power of 0.80.
In addition, lack of randomization, too few infants of seronegativity, recruitment of 2 groups from 2 hospitals and lack of groups receiving irradiated-only and filtered-only blood products may have limited our ability to conclude on what intervention is important.
In conclusion, the results from this pilot study suggests that filtering or irradiation of CMV seropositive blood products including PRBC and platelets did not significantly reduce transfusion-associated CMV infection among VLBWI in hyperendemic area and even if they acquired the infection, the impact of its illness is not as serious as those CMV seronegative recipients. Further validation is warranted in a larger cohort of infants.




 XML Download
XML Download