

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Thrombocytopenia (TP) is a frequent complication after allogeneic stem cell transplantation (SCT) (1-3). The prognostic significance of the platelet count in patients with chronic graft-versus-host disease (GVHD) has already been emphasized by several studies (3-6). In addition, persistent TP is regarded as a poor prognostic factor in transplant patients with chronic GVHD (3, 6). Bolwell et al. (7) also recently reported that the platelet count at day +100 was strongly associated with survival after allogeneic bone marrow transplantation (BMT).
Various multi-factorial causes may be related to the development of TP after allogeneic SCT (2), including GVHD, graft-failure, drugs (e.g. ganciclovir, cyclosporin A, FK-506, mycophenolate mofetil, trimethoprim/sulfamethoxazole), veno-occlusive disease, cytomegalovirus infection, opportunistic infection, recurrence of the primary disease, or hemolytic uremic syndrome/thrombotic thrombocytopenic purpura (2). However, it is very difficult to decipher the precise etiology of TP during the post-transplant period in a clinical setting. Even, the presence of TP itself after allogeneic SCT may impact on survival in transplant patients, regardless of the cause. Accordingly, the current study examined the platelet count at day +60 to stratify patient groups according to the platelet count, regardless of the etiology of TP, in an allogeneic peripheral blood stem cell transplantation (PBSCT) setting.
MATERIALS AND METHODS
Transplantation procedure
Sixty-three consecutive adult patients who had undergone allogeneic PBSCT (total 75 patients) and were evaluable on day +60 at Kyungpook National University Hospital (Daegu, Korea) between August 1998 and October 2003 were included in this retrospective study. The enrolled hematological diseases included acute myeloid leukemia (AML) (n=32), aplastic anemia (AA) (n=9), chronic myeloid leukemia (CML) (n=8), acute lymphoblastic leukemia (ALL) (n=5), lymphoma (n=3), myelodysplastic syndrome (MDS) (n=2), myeloma (n=2), paroxysmal nocturnal hemoglobinuria (PNH) (n=1), and metastatic colon cancer (n=1) with 34 (54%) standard-risk and 29 (46%) high-risk diseases. The median age of the patients was 37.0 yr (range, 16-56 yr), and the male to female ratio was 63:37% (n=40/23). The conditioning regimens consisted of a BuCy-based (n=40), Cy/anti-thymocyte globulin (ATG) (n=9), and fludarabine-based regimen (n=13). Myeloablative and reduced-intensity conditioning was adopted in 45 and 18 patients, respectively. All patients received peripheral blood stem cells (PBSC)s mobilized with 10 µg/kg/day G-CSF (Filgrastim, Leukokine®, CJ, Co., Seoul, Korea) alone (n=11), 10 µg/kg/day GM-CSF (Sargramostim, Leucogen®, LG, CI., Seoul, Korea) alone (n=10), a combination regimen (n=42) of 5 µg/kg/day G-CSF and 5 µg/kg/day GM-CSF for 4 or 5 days from 59 HLA-matched sibling donors (93.7%) and 4 mismatched sibling donors (6.3%), as previously reported (8, 9). The leukapheresis was performed using a Fenwal CS 3000+® blood cell separator (Baxter, Healthcare, Deerfield, IL, U.S.A.) with acid-citrate-dextrose as the anti-coagulant (10). In the case of the 4 mismatched transplants, 3 patients received unmanipulated PBSCs, while 1 patient received CD34+ cell selected PBSCs. For successful transplantation, the minimum target number of mononuclear cells (MNC)s and CD34+ cells was >3×108/kg and >3×106/kg, respectively. An ATG infusion was conducted in 9 patients (14.3%) as a part of the Cy/ATG conditioning and in 6 patients (9.5%) as part of the reduced-intensity conditioning.
The prophylaxis against acute GVHD consisted of methotrexate (MTX) and cyclosporin A (CSA; Cipol-N®, ChongKunDang, Seoul, Korea), except for 2 cases that used CSA/mycophenolate mofetil (MMF; n=1) or CSA/MTX/MMF (n=1). The infection prophylaxis consisted of ciprofloxacin (250 mg twice a day orally [p.o.])/metronidazole (500 mg three times a day p.o.)/fluconazole (100 mg once a day p.o.), beginning with the initiation of conditioning, and acyclovir (600 mg twice a day p.o.) from day-1 until day+180. Cotrimoxazole was started after engraftment, and ursodeoxycholinic acid was used for the veno-occlusive disease prophylaxis, beginning with the initiation of conditioning. Intravenous immunoglobulin (500 mg/kg) was infused every two weeks until day+100, then every month until +6 months. All patients received irradiated blood products that had been depleted of leukocytes using filters.
Definitions
The day of the stem cell infusion was defined as day 0. Engraftment was confirmed by peripheral blood counts (myeloid: peripheral absolute neutrophil count of more than 0.5×109/L, megakaryocyte: peripheral platelet count of more than 20×109/L for at least 3 consecutive days without requiring transfusion). Overall survival (OS) was defined as the time from transplantation until death from any cause. Disease-free survival (DFS) was defined as the time from transplantation until relapse or death in complete remission (CR), by whatever cause. The relapse incidence was defined as the time from transplantation until relapse. Non-relapse mortality (NRM) was defined as the time from transplantation until death from infectious or GVHD-related causes. The day of an infectious event was defined as the day when the clinical symptom(s) or sign(s) of infection was first reported. The causative organisms were identified by microbiologic or histologic methods. High-risk diseases were defined as acute leukemia that was more than the first CR or with extramedullary involvements, Ph+ acute lymphoblastic leukemia, advanced phase chronic myelogenous leukemia, or primary refractory or multiple relapsed malignancies. Acute and chronic GVHD were diagnosed and graded using established criteria (11, 12). Positive cytomegalovirus (CMV) antigenemia was defined as any positive level in a CMV pp65 antigenemia assay. CMV disease was defined as a symptomatic CMV infection. According to the platelet count at day +60, the patients were classified into 3 groups. Group 1: platelet count ≤29×109/L, Group 2: platelet count 30-79×109/L, Group 3: platelet count ≥80×109/L.
Statistics
The clinical characteristics and transplant outcomes of the stratified groups were compared using Fisher's exact test or Kruskal-Wallis's test. Survival analyses of OS, DFS, the relapse incidence, incidence of NRM, and infectious events were conducted using the Kaplan-Meier method. A log rank test was also used for a survival analysis. Multivariate analyses of Cox's proportional hazard regression were applied to define the risk factors for OS, DFS, the relapse incidence, and incidence of NRM and infectious events using the backward method. The variables included for the multivariate analyses were as follows: the group according to the platelet count at day +60, the age of patients, CD34+ cell counts (<6 vs. ≥6×106/kg), conditioning (reduced-intensity conditioning vs. myeloablative), donor status (HLA-matched sibling donors vs. alternatives), disease status (standard- vs. high-risk), the use of ATG (yes vs. no), acute GVHD (grade 0, 1 vs. grade 2-4), and chronic GVHD (yes vs. no). A cut off p-value of 0.05 was adopted for all statistical analyses. The statistical data were obtained using an SPSS software package (SPSS 10.0 Inc. Chicago, IL, U.S.A.).
RESULTS
Patient characteristics
The patients' characteristics are summarized in Table 1. Out of the total 63 patients, 10 patients (15.9%) were classified in group 1 (platelet count ≤29×109/L), 23 patients (36.5%) in group 2 (platelet count 30-79×109/L), and 30 patients (47.6%) in group 3 (platelet count ≥80×109/L). No differences in the pre-transplant characteristics were found among the 3 groups, except for the mobilization regimens (p=0.051), where the GM-CSF alone mobilization regimen was associated with a lower platelet count at day +60 compared with the GM-/G-CSF combination regimen (p=0.038). The median doses of CD34+ cells and MNC infused were 7.37×106/kg (range 0.69-20.60) and 8.10×108/kg (range 1.69-22.30), respectively. No difference in the MNC dose was noted among 3 groups, yet an association between the CD34+ cell dose and the different groups was found, although with a marginal significance (Table 1).
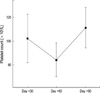
Measurement of platelet count at day +30, +60, and +90
The serial measurements of the platelet count revealed a drop-and-rise pattern of platelet recovery from day +30 to day +90 (Fig. 1). The mean platelet count at day +30, +60, and +90 was 102.254 (95% confidence interval [C.I.] 81.820-122.688), 84.302 (95% C.I. 70.115-98.488), and 111.281 (95% C.I. 94.279-128.283)×109/L, respectively.
Transplantation outcomes
The median engraftment day for neutrophils and platelets was 15 days (range, 9-30 days) and 14 days (range, 9-81 days), respectively. Eventually, 54 patients (85.7%) achieved a stable platelet engraftment (platelets≥50×109/L) with a median of 27 days post-transplant (range, 11-396 days). Forty-nine (77.8%) out of the total 63 patients experienced acute GVHD over grade 1 (29 patients: grade 2 acute GVHD, 14 patients: grade 3, 4 acute GVHD), while 40 (70.2%) out of evaluable 57 patients experienced chronic GVHD and 19 patients (33.3%) extensive chronic GVHD.
When last assessed with a median follow-up duration of 340 days (range 56-1,839 days; 755 days among survivors with range of 107 to 1,839 days), 22 relapses (34.9%) and 31 deaths (49.2%), including 16 NRM cases (25.4%), were recorded. The causes of death included relapse (n=15, 48.4%), infection (n=12, 38.7%), and GVHD-related death (n=4, 12.9%). The 1- and 3-yr OS rates were estimated as 49.0±6.0% and 43.2±6.2%, respectively, while the 1- and 3-yr DFS rates were estimated as 40.1±5.9% and 35.9±6.0%, respectively. The cumulative incidence of relapse after 1 and 3 yr was estimated as 39.4±6.6% and 42.8±7.0%, respectively, while that of NRM after 1 and 3 yr was 34.9±6.1% and 40.3±6.6%, respectively. The cumulative incidence of overall infectious complications beyond day +60 (n=31) was 19.7±4.7% on day +100 and 44.5±6.5% on day +365. The median onset of infectious complications after day +60 was 176 days post-transplant (range 63-704 days). The cumulative incidence of bacterial complications (n=19) was 15.5±4.3% on day +100 and 26.7±5.7% on day +365, while that of viral infection (n=12) was 3.8±2.0% on day +100 and 18.1±5.6% on day +365, and that of fungal infection (n=3) was 1.7±1.6% on day +100 and 6.3±3.6% on day +365.
Outcomes according to platelet count at day +60
The transplantation outcomes according to the platelet count at day +60 are summarized in Table 2. Differences were noted in the incidence of severe acute GVHD (grade 3, 4; p=0.001) and extensive chronic GVHD (p=0.013) among the 3 groups. Group 1 showed a higher incidence of severe acute GVHD (50% for group 1 vs. 30% for group 2 vs. 7% for group 3) and extensive chronic GVHD (67% for group 1 vs. 43% for group 2 vs. 20% for group 3) compared to the other 2 groups.
Meanwhile, group 3 was associated with a significantly better 3-yr OS (60.3±9.9% for group 3 vs. 45.8±11.3% for group 2 vs. 13.3±12.0% for group 1, p=0.0030, Fig. 2A) and DFS (48.7±10.0% for group 1 vs. 41.7±11.3% for group 2 vs. 15.0±12.8% for group 1, p=0.0076). There was no difference in the relapse incidence among the 3 groups (51.3±9.9% for group 1 vs. 23.7±9.5% for group 2 vs. 40.0±19.7% for group 1, p=0.2825), while group 3 was associated with a lower 3-yr NRM rate (11.1±7.5% for group 3 vs. 42.8±12.6% for group 2 vs. 84.0±14.2% for group 1, p<0.0001, Fig. 2B).
In the analysis of the causes of death, there was no difference in the mortality due to disease progression among the groups, yet a distinct difference in the mortality due to NRM (Table 2). Ten percent of group 3 died of NRM, while 30% and 60% of groups 2 and 1 died of NRM, respectively (p=0.005). The cause of NRM was shown in Table 2.
Multivariate analyses
The results of the multivariate analyses for prognostic factors are shown in Table 3. In terms of OS, the stratified groups according to the platelet count at day +60 were identified as an independent prognostic factor (p=0.003) together with the CD34+ cell dose (p=0.001), disease risk (p<0.001), and development of chronic GVHD (p<0.001). For NRM, the stratified groups were also identified as an independent prognostic factor (p=0.003) together with the CD34+ cell dose (p<0.001), disease risk (p=0.004), and development of acute GVHD (p=0.033). Furthermore, the results of the multivariate analyses for the cumulative incidence of infectious events identified that the stratified groups according to the platelet count at day +60 were an independent prognostic factor (p=0.047) together with the CD34+ cell dose (p=0.026).
DISCUSSION
TP is known to have a prognostic significance in patients receiving allogeneic SCT (1-3). The most important mechanism involved in the development of TP after allogeneic SCT is a GVHD-related event, including autoimmune (ITP-like) destruction, immune regulation, or viral-induced suppression of platelet production. Anasetti et al. (13) reported that TP developed most frequently secondary to increased platelet destruction mediated by platelet auto-antibodies in an allogeneic setting. Meanwhile, Nash et al. (2) reported an association with delayed platelet recovery in two common situations (GVHD and infection) after allogeneic SCT, causing a decreased platelet survival in the peripheral circulation. They also proposed that elevated cytokines, including G-CSF, M-CSF, IL-1α, IL-1β, and IL-6, may contribute to the activation of monocytes and macrophages that are critical components for the elimination of platelets. As such, cytokine-induced thrombocytopenia could offer another explanation for platelet consumption after allogeneic SCT as an non-autoimmune mechanism (2).
First et al. (1) previously described two distinct thrombocytopenic syndromes, transient and persistent TP. Transient TP, where a normal platelet count (>100×109/L) is initially established by day +40, which then diminishes to <10 to 45×109/L on day +40 to +70 with subsequent resolution of the TP by day +90, has no adverse affect on the prognosis, whereas persistent TP, where a platelet count >100×109/L is not achieved at any time during the first 4 months post-transplant, carries a high mortality and high association with both severe acute and chronic GVHD. During the post-transplant period until day +100, several clinical events predisposing the development of TP tend to occur simultaneously, thus, it is very important to decipher the precise etiology of TP in the post-transplant period. In the current study, day +60 was adopted as a landmark day to determine the prognostic role of the platelet count after allogeneic SCT, as day +60 effectively reflects the "dip period" of the platelet count (day +40-day +70) in terms of post-transplant platelet recovery (1). As such, it was found that TP at day +60 was associated with the prognosis of patients in terms of NRM and infectious events, opportunistic infections, and an association with severe acute GVHD and extensive chronic GVHD, regardless of the etiology of TP. Therefore, this finding implies that the platelet count at day +60 can play a prognostic role for patients receiving allogeneic SCT and reflect the probability of infectious events and NRM, even before the development of chronic GVHD.
The use of PBSC is associated with less regimen-related toxicity and earlier hematologic recovery without an increase in acute GVHD, yet concerns remain in relation to chronic GVHD adversely affecting OS and NRM (14). In a study by Przepiorka et al. (14), the incidence of clinical extensive GVHD in allogeneic PBSCT was 67%, which was higher than that in allogeneic BMT. As such, the incidence of TP (80×109/L) may also be anticipated to be higher in relation to GVHD in an allogeneic PBSCT setting than in a BMT setting. In the current study on allogeneic PBSCT, the incidence of chronic GVHD and TP was relatively high compared with previous reports on allogeneic BMT. This disadvantage can be translated into frequent use of intensive immunosuppressions for profound GVHD, which in turn can increase the incidence of infectious events. In the present study, the most common cause of NRMs was opportunistic infection in thrombocytopenic patients (50% vs. 26% vs. 3%; Table 2). According to Bolwell et al. (7), thrombocytopenic patients at day +100 after allogeneic BMT had a far lower risk of dying of infection than dying of GVHD. However, in trials with allogeneic PBSCT, the incidence of extensive chronic GVHD has been found to be higher than that in a BMT setting, thereby facilitating the use of more intensive immunosuppressive therapy that has adverse effects on the incidence of opportunistic infection and NRM. As such, in an allogeneic PBSCT setting, more effort is needed to predict high-risk patients in terms of chronic GVHD and opportunistic infection than in a BMT setting. Accordingly, measuring the platelet count at day +60 would appear to be a simple method for stratifying patients according to their risk of chronic GVHD, infection, and NRM.
However, the caution is needed in the interpretation of the current study. More inclusion of the patients with aplastic anemia into group 2 or 3 than group 1 might influence on the outcomes, even though statistically insignificant (p=0.387). Accordingly, further study will be needed to reach a clear conclusion on this issue with homogeneous disease population.
TP after allogeneic SCT is a worrisome problem requiring significant care. Available practices to manage TP after allogeneic SCT include preventing or treating the precipitating factors increasing the consumption or destruction of platelets, such as GVHD or infection. Bolwell et al. (7) recommended more intensive immunosuppressive treatment or alternative GVHD clinical trials for patients with TP and ongoing GVHD in the absence of active infections. In addition, given the results of the current study, infection surveillance or prophylaxis with antibiotics or antifungal agents may also be beneficial for patients with TP at day +60 post-transplant.
In conclusion, measuring the platelet count at day +60 is a simple method for predicting the risk of chronic GVHD development and the prognosis of recipients in terms of OS and NRM after allogeneic PBSCT. Patients with TP at day +60 were found to have a higher risk of NRM and infectious events that had an adverse affect on long-term survival after allogeneic PBSCT.




 XML Download
XML Download