

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hematopoietic stem cell transplantation (HSCT) has been increasingly used to treat patients with malignant, non-malignant hematologic disorders and severe autoimmune diseases over the last 3 decades (1). Numerous advances have taken place in the field of HSCT to make the procedure safer. In addition, better supportive care measures have been incorporated into practice, such as hematopoietic growth factors to accelerate neutrophil recovery, new, more potent antimicrobial agents and prophylaxis strategies to prevent infection. These advances have resulted in better overall outcomes and have increased the safety of the procedures that in turn enable more patients to be eligible for HSCT. Despite theses advances, infectious complications remain a major cause of transplant related morbidity and mortality (2). There are several risk factors for infection that still exist in HSCT patients; the intensity of the conditioning regimen and the type of HSCT, which influence the development of graft-versus-host disease (GVHD) and the rate of immune reconstitution (2, 3).
Recently, HSCT from alternative donors such as matched unrelated donor (MUD) and mismatched related donors as well as non-myeloablative HSCT have increased at Catholic HSCT Center (4). Therefore, a wide range of patients including elderly patients, patients with advanced diseases, or with autoimmune diseases, could have received HSCT. In accordance with the changes in HSCT, infectious complications following HSCT have changed recently. In the present study, we analyzed the recent trends of infectious complications and outcomes following HSCT in a single institution.
MATERIALS AND METHODS
Patients
We reviewed retrospectively the medical records of all consecutive 379 adult patients who underwent HSCT at the Catholic HSCT Center from January 2001 to December 2002. The end point of the study was set to September 2004 or time of death or follow-up loss.
Conditioning regimen and GVHD prophylaxis
Two hundred ninety seven patients (78.4%) received total body irradiation (TBI) as a part of conditioning and additional cytoreductive agents consisting of cytarabine, cyclophosphamide, or busulfan. The other patients received non-TBI based conditioning regimen, consisting of fludarabine, mephalan, busulfan, cyclosphosphamide, procarbazine, or anti-thymocyte globulin (ATG). Sixteen patients received a conditioning regimen of reduced intensity. Prophylaxis of GVHD was cyclosporin A with short course methotrexate with or without IL-2, tacrolimus with cyclosporin A or short course methotrexate (Table 1).
Supportive care and antimicrobial prophylaxis
All patients were nursed in laminar airflow and high-efficiency particulate air (HEPA)-filtered rooms until engraftment. Intravenous access was achieved with a double-lumen tunneled central venous catheter. Transfused blood products were irradiated and leukocyte-depleted. All patients received oral ciprofloxacin 500 mg daily as antibacterial prophylaxis. Antifungal prophylaxis included fluconazole 50 mg (for autologous transplant recipients) or itraconazole 200 mg per os (p.o.) daily (for allogeneic transplant recipients). Trimethoprim/sulfamethoxazole (80/400 mg p.o. daily) for Pneumocystis pneumonia prophylaxis was given from engraftment until posttransplant 6 months or more if GVHD were present. Acyclovir (800 mg p.o. daily) given from -7 to engraftment was followed by long-term low-dose (200 mg p.o. daily) administration until 6 months posttransplantation. For cytomegalovirus (CMV) prophylaxis, high dose acyclovir (10 mg/kg i.v. thrice daily) or ganciclovir (5 mg/kg intravenous (i.v.) twice daily) with or without CMV immunoglobulin was administered to patients who received MUD HSCT or haploidentical HSCT respectively.
Definition of terms
Fever was defined as a single oral temperature of ≥38.3℃ or temperature of ≥38℃ for ≥1 hr. Neutropenia was defined as absolute neutrophil count (ANC) of less than 500/µL or less than 1,000/µL with predicted decline to 500/µL within the next 2 days. Infections in febrile neutropenia were classified in accordance with the recommendations of the Infectious Diseases Society of America (IDSA) (5) as follows: microbiologically documented infection (MDI), when a clinically significant pathogen was identified from normally sterile specimen or from an affected site by culture or biopsy; clinically documented infection (CDI), when fever was accompanied by appropriate clinical findings; unexplained fever (UF) when there was no clinical, radiological, or microbiological evidence of infection.
Invasive fungal infection (IFI) was defined as possible, probable, or proven, according to the published consensus criteria (6). CMV infection was defined as isolation of CMV or detection of viral proteins or nucleic acid in any body fluid or tissue specimen. CMV end-organ diseases were defined according to definitions presented in the previous literature (7).
Acute GVHD was defined and graded according to the standard criteria (8). Chronic GVHD was assessed as being absent, limited, and extensive, as previously described (9). Engraftment was defined as an ANC ≥500/µL on 3 consecutive days or established by bone marrow biopsy.
Patients were classified into 2 groups according to the disease status at the time of transplantation. Standard-status group included cases of acute leukemia in the first remission, chronic myelogenous leukemia (CML) in the first chronic phase, myelodysplastic syndrome (MDS) with refractory anemia (RA) or RA with ringed sideroblasts and severe aplastic anemia (SAA) with a history of less than 20 pints of transfusions before transplantation. The advanced-status group included acute leukemia in second remission or relapse, the accelerated phase or blast crisis of CML or CML in the second chronic phase, MDS (refractory anemia with excess blasts [RAEB] or RAEB in transformation), non-Hodgkin's lymphoma (NHL), and SAA with over 20 pints of transfusions before transplantation (10).
Antibiotic treatment
An empirical antibiotic regimen was given to febrile neutropenic patients according to the strategies of Catholic HSCT Center that was modified from the IDSA guideline (5). Febrile neutropenic patients were initially treated with ceftazidime (2 g i.v. twice daily) or cefepime (2 g i.v. twice daily) in combination with amikacin (750 mg, single daily). Glycopeptide and conventional or liposomal amphotericin B were sequentially added as a part of multi-step strategies if patient remained febrile for 3-5 days after the start of initial therapy. If the clinical status of patients deteriorated, initial antibiotics regimen was replaced by carbapenem. Whenever the clinical status was deteriorating, modification was done earlier. In patients with MDI, therapy was modified, if necessary, according to the results of susceptibility test.
CMV antigenemia assay for pp65 antigen in leukocytes was performed after engraftment. If CMV antigenemia was positive (≥5 positive cells/200,000 leukocytes for low risk group, ≥1 positive cells/200,000 leukocytes for high risk group), pre-emptive ganciclovir was administered (5 mg/kg i.v. twice daily) until 2 consecutive negative assays or more than 3 weeks (10).
Data collection and analysis
Baseline information included age, sex, underlying diseases, disease status at the time of transplantation, the type of donor, and the intensity of conditioning regimen.
We reviewed and analyzed the clinical and microbiological features of recipients in the context of three risk phases following HSCT, that is, pre-engraftment period (from the day of the transplant to engraftment, approximately day 30), mid-recovery period (from engraftmemt until day 100), and late-recovery period (from day 100 until the patient regains normal immunity).
We used χ2-test or the Fisher's exact test for the analysis of categorical variables and the Student t-test for continuous variables. We evaluated risk factors affecting mortality by univariate and multivariate logistic regression analysis. A p-value <0.05 was accepted as statistically significant.
RESULTS
Clinical characteristics
The median age of 379 recipients was 33 yr (range:15-61) with the ratio of male to female 203:176. Acute myelogeneous leukemia (AML) was the most common underlying disease (n=151, 39.8%) followed by acute lymphocytic leukemia (ALL), CML, SAA, and others including 11 cases of severe autoimmune diseases.
A total of 287 patients received allogeneic HSCT from MSD (n=211, 55.6%), MUD (n=66, 17.4%), and haplotype mismatched related donors (n=7, 1.8%). The others received autologous HSCT (n=92, 24.3%).
The source of stem cells was bone marrow (BM) in 232 cases (61.2%), peripheral blood stem cells (PBSC) in 96 cases (25.3%), BM plus PBSC in 49 cases (12.9%), and cord blood in the remaining 2 cases (0.5%).
Median time to engraftment was 15 days (range, 6-126). There were four cases of graft failures and one of them received bone marrow reinfusion and engrafted. However, all patients with graft failure died due to infectious and/or other complications. The more detailed patient characteristics are summarized in Table 1.
Infections during the preengraftment period
Two hundred and thirty two patients (61.2%) developed 288 febrile episodes during hospitalization. Among 288 episodes, 70 (24.3%) were MDI, 160 (55.5%) were CDI, and 58 (20.1%) were UF. The median time to development of fever was 6 days after HSCT (range: -4~9 days) and the mean duration of therapeutic antibiotics was 15.8±9.8 days. The oropharynx was the most common site of infection and the second most common site was the gastrointestinal tract, followed by the lower respiratory tract, the skin and soft tissue, and primary bacteremia successively (Table 2). A total of 92 organisms were identified during the pre-engraftment period. Bacterial pathogens accounted for 78.3% (72/92) of the MDI. Overall, the proportion of Gram-negative bacteria was much higher than that of Gram-positive bacteria (51.1% vs. 27.2%, respectively) Escherichia coli was the predominant pathogen followed by Staphylococcus spp. (9 coagulase-negative staphylococci, 2 S. aureus), Streptococcus spp. (5 alpha-hemolytic streptococci, 3 S. mitis, 1 beta-hemolytic Streptococcus), and Enterococcus spp. (4 E. faecium, 2 E. faecalis) (Table 3). There were 32 cases of invasive fungal infection (IFI), in which only one case was proven to be Aspergillus spp. infection, and the others were possible IFI. Candida infection did not occur in any cases. Twelve patients died during pre-engraftment period, and seven of them died of infection (7/12, 58.3%). There were 3 cases of graft failure among the dead (3/12, 25%).
Infections during the mid-recovery period (from engraftment until day 100)
Because 12 out of 379 patients died before engraftment, 367 patients in the mid recovery period were analyzed. Overall, 70 patients had infectious complications requiring hospitalization, and a total of 76 infection episodes developed. The skin and soft tissue and lower respiratory tract were the most common sites of infection (Table 2). Viral infections were predominant and accounted for 77.8% of pathogens isolated (Table 3). Herpes viruses (25 varicella-zoster viruses [VZV], 4 Cytomegalovirus [CMV], 2 Epstein-Barr virus [EBV], 1 Human herpes virus-6 [HHV-6]) were the most common pathogens. There was a case of meningoencephalitis caused by HHV-6 and 2 cases of EBV-associated posttransplant lymphoproliferative disorders (PTLD). In this period, IFI developed in 9 patients (9/367, 2.5%), which were one case of paranasal aspergillosis confirmed by histopathology and 8 cases of possible IFI. Among 76 episodes, the skin and soft tissue infections (n=26, 34.2%), which included chicken pox and herpes zoster, was most predominant followed by the lower respiratory tract infection.
During the early post-transplant period (pre-engraftment and mid-recovery periods), there were a total of 17 cases of virus-associated hemorrhagic cystitis including BK virus in 11 cases, adenovirus in 2, JC virus in 1, adenovirus plus BK virus in 1, and BK virus plus JC virus in 2 cases.
Twenty eight patients died during the mid-recovery period, and 15 of them died of infection (15/28, 53.6%). There was one case of follow-up loss. The underlying hematological malignancies were relapsed in 3 cases among the dead (3/28, 10.7%).
Infections in the late-recovery period (from day 100)
Out of 367 patients, 28 patients died during the midrecovery period and one patient was lost during the follow-up. Three hundred thirty three patients were analyzed. A total of 154 patients had infectious complications, and 228 episodes of infection developed. The most common site of infection was the lower respiratory tract (42.1%, 96/228), followed by the skin and soft tissue, which included chicken pox and herpes zoster (Table 2). About 26.2% (96/367) of recipients experienced VZV infection after transplantation (25 in mid and 74 in late recovery period), which consisted of 11 chicken pox, and 88 herpes zoster. Among the 88 patients of herpes zoster, 3 patients had relapsed herpes zoster and 7 patients had disseminated herpes zoster. The seropositivity for CMV was very high before allogeneic HSCT in both recipients (n= 275, 96.8%) and donors (n=276, 97.5%). Overall, CMV antigenemia occurred in 161 recipients who underwent allogeneic HSCT (161/287, 56%), and 11 patients developed CMV diseases (pneumonia 8; colitis, 1; retinitis 2). Median time to CMV diseases was 162 days after transplantation (range, 39-724 days). There were 27 cases of IFI (27/338, 7.98%) which included 2 proven, 3 probable, and 22 possible cases and fungi were the second most common pathogens during this period. Pneumocystis pneumonia occurred in 3 patients (0.8%, 3/367). During the mid and late recovery period, the incidence of tuberculosis in 2.1% (8/367), and 2 of them died directly due to pulmonary tuberculosis.
Clinical outcome and risk factor
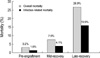
Fourteen cases were lost during the follow-up period (1 in mid-recovery period, 13 in late-recovery period) and all of them had underlying diseases relapsed. They were presumed to be dead and counted as deaths. The mortality rate during pre-engraftment period was 3.2% (12/379) and among the 12 deaths, 7 deaths (58.3%) were attributable to infection; four patients had pneumonia and three had septic shock. The mortality during mid-recovery period was 7.9% (29/367) and 15 deaths (51.7%, 15/29) were attributed to infection; 12 patients had pneumonia, 2 had hemorrhagic cystitis and 1 had fulminant hepatitis B. In the late-recovery period, the mortality rate was 26.9% (91/338), and 59.3% (54/91) of these deaths were related to infection; 42 patients with pneumonia, 7 with septic shock, 1 with necrotizing fasciitis, 1 with cerebral aspergillosis, and 3 with fulminant hepatitis B. Among the deaths after engraftment, 72 cases had underlying diseases relapsed (3 in mid-recovery period, 68 in late-recovery period). (Table 4, Fig. 1).
By univatiate analysis, risk factors for infection-related mortality in accordance with the periods and types of HSCT, are summarized in Table 5. Multivariate analysis showed that risk factors for infection-related mortality were as follows; during pre-engraftment period, fungal infection and septic shock; during the mid-recovery period, presence of hemorrhagic cystitis and delayed engraftment were significantly important, and transplantation from alternative donors (unrelated or haplotype mismatched related donors), although statistically not significant, had a trend to infection-related death (p=0.06); during the late-recovery period, fungal infection, presence of chronic GVHD, and relapse were significantly important risk factors in allogeneic HSCT. Relapse of underlying disease and fungal infections were the significant risk factors following autologus HSCT.
DISCUSSION
In this study, we focused on the recent trends and clinical outcomes of infectious complications in accordance with the changes in HSCT from January 2001 to December 2002. When compared with the previous reports at the same center (11-13), there were several changes in HSCT. First, the proportion of HSCT from unrelated matched donors had increased. Second, the spectrum of patients was more widened because NST for elderly or high risk patients who were vulnerable to treatment related mortality, and transplantations from haplotype mismatched related donors were introduced and performed increasingly. And also, refractory autoimmune disorders were tried to treat by use of autologous HSCT (4). All of the above changes put the recipients under more profound, prolonged immunosuppression for prevention and treatment of GVHD, and for controlling underlying disorders in case of autoimmune disorders.
During the pre-engraftment period, the proportion of MDI and CDI had become larger than that of the past (43% in between 1993 and 1999 vs. 79.8% between 2001 and 2002) (4, 11-13). Among MDI, bacterial pathogens accounted for 85.6%. In contrast to the previous studies from other countries, which identified that Gram positive cocci (GPC) were the predominant pathogens (3, 4, 14), the most common cause of bacteremia had been Gram negative bacilli (GNB) rather than Gram positive cocci (GPC) at the Catholic HSCT center and E. coli had been the most frequently isolated during the last decade (4, 11, 12). In the present study, E. coli was still the most common cause of MDI. We conducted antimicrobial prophylaxis using ciprofloxacin since 1995. However, quinolone prophylaxis did not decrease the incidence of GNB infection but increased that of quilonolone-resistant E. coli (76.6%, 26/32) (data not shown here), which had become a major concern at the Catholic HSCT center (15, 16). Although the efficacy of ciprofloxacin prophylaxis was still controversial (16-18), we continued to use ciprofloxacin prophylaxis on the basis of two reasons. First, despite the emergence of quinolone resistance in E. coli, cross-resistance to β-lactam, especially 3rd generation cephalosporin and aminoglycoside, was rare and mortality rate due to quinolone resistant E. coli was low (13, 19). Second, the incidence of the most stains of GNB other than E. coli, such as P. aeruginosa, decreased and they remained susceptible to ciprofloxacin (15, 16). Despite the predominance of GNB infections, the incidence of GPC infections among bacterial pathogens were continuously increasing during the past decade from 25.0% (8/32) during the early 1990s to 34.7% (25/72) in the present study (11-13). Among Gram positive organisms, a trend in dominant pathogens had been changing from Staphylococcus spp. to Streptococcus spp. and the ratio of streptococci to staphylococci was increased from 5:13 in the late 1990s to 9:9 in the present study. Severe mucositis due to intensive conditioning regimen using TBI, and use of ciprofloxacin as antimicrobial prophylaxis could be possible explanations for this change (20). Fludarabine, as well as cytarabine, was reported to be associated with streptococcal bacteremia (20). Therefore, increasing use of fludarabine-based conditioning regimens could lead to the shift to streptococcal infection in the future. Considering all of the changes described above, a question whether we should continue ciprofloxacin or not, is raised and further assessment of the effectiveness of quinolone prophylaxis is warranted.
As patients remain functionally and quantitatively deficient in T and B lymphocytes even after full hematopoietic reconstitution during the post-engraftment period (2, 3), the patterns of infection are quite different from those of the preengraftment period. In this study, viral infections, especially VZV and CMV, were the main problem during mid and late recovery period and this pattern of infectious complications was not changed from the past (4, 12, 13). However, compared to the previous report in the late 1990s, the overall incidence CMV infections in recipients of allogeneic HSCT was increased from 35% to 56%, but in contrast, the incidence of CMV disease decreased from 6.5% to 3.8% (11/287) (4, 12, 13). CMV diseases tended to develop in late recovery period. The low incidence but late occurrence could be partly due to the effect of risk-adaptive preemptive ganciclovir therapy guided by CMV antigenemia (10, 21). However, it should be taken into consideration that there was no difference in the incidence of CMV disease with or without preemptive therapy (10), and CMV antigenemia did not always precede CMV disease. Therefore, we needed the more sensitive method to detect CMV reactivation, and recently, we adopted real-time polymerase chain reaction for detection and quantification of CMV infection. And, further study to compare the efficacy of diagnostic methods to prevent CMV disease will be warranted.
There were only 3 cases of microbiologically proven Pneumocystis pneumonia (0.79%, 3/367). Its incidence was remarkably decreased compared to the previous report in the late 1990s at this center (6.5%, 15/230) (13, 22). The more strict application of sulfamethoxazole/trimethoprim prophylaxis in allogeneic HSCT recipients seemed to be effective for prevention of Pneumocystis pneumonia. Pneumocystis pneumonia developed in late recovery period and two of them occurred at more than 6 months after transplantation. Although its incidence was low, there were 9 cases of radiologically suspected Pneumocystis pneumonia who were treated with sulfamethoxazole/trimethoprim. Three patients who received autologous PBSCT developed Pneumocystis pneumonia (2 suspicious cases and 1 confirmed case) in this study. Therefore, sulfamethoxazole/trimethoprim prophylaxsis should be considered not only for the patients who received allogeneic HSCT but also those who received autologus HSCT with risk factors, and duration of this prophylaxis should be extended as long as chronic GVHD is resolved or immunosuppressants are discontinued (23, 24).
The mortality rate during the pre-engraftment period tended to decline during the past decade thanks to the improvement of peri-transplantation procedures and supportive care (7.6% in the early 1990s, 4% in the late 1990s and 3.2% in the early 2000s) (4, 11-13). As more patients survived after engraftment, the infectious complications after engraftment became more important. Infectious complications were most common during the pre-engraftment period followed by the late-recovery, and mid-recovery period successively. However, mortality rate was highest during the late-recovery period and the proportion of infection-related death was similar in all three periods, which indicated that the more patients died directly due to infectious complications during the late recovery period and infection was a still important matter in managing transplant recipients after recovery of neutropenia. This trend had started to become apparent since the late 1990s because transplants from alternative donors such as unrelated donors or family mismatched donors had started to be performed at that time and used increasingly. Among the risk factors attributable to infection-related mortality, IFI was the statistically significant, independent factor in both pre-engraftment and late recovery periods and during the early and late recovery periods, was the presence of GVHD after allogeneic HSCT. The timing of IFI was bimodal distribution in this study, with peak that was correlated with neutropenia (pre-engraftment) and GVHD (late recovery period). Prolonged neutropenia before engraftment is well known as an absolute risk factor for IFI. The presence of GVHD and subsequent immunosuppression after engraftment are also established risk factors (25-27). The shift from early to late post-engraftment IFI may be affected by neutrophil dysfunction in the setting of GVHD and corticosteroid administration, an increase in the proportion of patients who are alive late after engraftment thanks to the advance of supportive measure, and increase in the proportion of transplantations from unrelated donors or mismatched siblings, which require more immunosuppression to prevent rejection and GVHD. And also CMV infection could affect this shift although mechanism to explain the association between CMV infection and fungal infections are unknown (25-27).
Now, we could say that it is important how to manage not only the patients with neutropenia but also the patients with GVHD. Recently, the potent immunosuppressive agents were used for the management of refractory severe GVHD and could become a major contributor to risk for Aspergillus infections (26). Alemtuzumab, anti-CD52 monoclonal antibody, that depletes peripheral blood T and B cells without affecting the stem cells, has increasingly come to be used in HSCT recipients for the management of GVHD as well as a part of the conditioning regimen, and conferred a significantly greater risk for fungal and CMV infections (26, 27). And its usage is expected to be increased. In accordance with the changing management of HSCT recipients after engraftment, a new strategy of risk adapted antifungal and antiviral prophylaxis should be made. Wingard suggested that continuation of antifungal prophylaxis was reasonable until the completion of the immunosuppressive treatment course or until immunosuppression is substantially reduced (28). However, duration of antifungal therapy and what kind of antifungals to be used as prophylaxis need to be evaluated and cautiously defined. We should develop and adopt the new methods for early detection of fungus, such as galactomannan enzyme immunosorbent assay (29) and nucleic acid sequence based amplification for invasive aspergillosis (30). And preemptive or prompt antifungal treatment guided by early diagnosis, should be done in high risk patients. For prevention of bacterial and viral infection, the more effective vaccination strategy which is the economic and easy way to prevent infections, should be established and strictly controlled.





 XML Download
XML Download