

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
E-cadherin is a cell-cell adhesion molecule which is anchored to the cytoskeleton via catenins and acts as a suppressor of tumor invasion and metastasis (1, 2). Reduced expression of E-cadherin has been associated with invasion and recurrence of hepatocellular carcinomas (HCCs) (3). Somatic mutations of E-cadherin are found in poorly differentiated breast and gastric cancers (4, 5) but have not been described to date in HCC. However, the allelic deletion of E-cadherin and neighboring loci (6) and the hypermethylation of E-cadherin (7) have been observed in HCCs.
DNA methylation is one of the best-understood epigenetic changes in human cancers. DNA methylation may play roles in carcinogenesis by virtue of 3 mechanisms: 1) DNA cytosine methylation facilitates gene mutation, as 5-methylcytosine is deaminated to thymine (8); 2) aberrant DNA methylation may be associated with allelic loss (9); and 3) DNA methylation occurs frequently in CpG islands near regulatory regions of genes and affects the transcriptions of specific genes (7). Promoter region CpG islands are protected from methylation in normal cells, excepting genes on the inactive X chromosome and imprinted genes (10). This protection is critical, since the methylation of promoter region CpG islands is associated with the loss of expression of these genes (11). CpG methylation has recently been shown to be an important mechanism in the transcriptional inactivation of E-cadherin (12), and CpG methylation around the promoter region of E-cadherin was found to be significantly correlated with reduced E-cadherin expression in HCCs (7). Recent studies reported that loss of heterozygosity (LOH) and promoter methylation of E-cadherin occurred in different stages of HCCs (6) and that promoter methylation of E-cadherin was more frequent in HCCs retaining both alleles of the gene than in LOH-bearing HCCs (13).
The two general explanations of the histogenesis of HCC are de novo hepatocarcinogenesis, namely cancer development directly from non-neoplastic hepatocytes, and multistep hepatocarcinogenesis. Dysplastic nodules (DNs) have been described as precancerous lesions in multistep hepatocarcinogenesis (14), i.e., DN progresses to DN with microscopic foci of HCC and then to HCC. Some cases of HCC may progress further to become more malignant, with the possibility of metastases. But, a few reports are available on the genetic and epigenetic changes of E-cadherin in DNs (15). Despite recent advances in diagnostic modalities and therapies, the long-term survival of HCC patients remains poor because of its high incidence of recurrence after initial treatment.
In this study, we investigated the methylation status of E-cadherin and E-cadherin protein expression in HCCs and DNs to clarify the significance of E-cadherin methylation in multistep hepatocarcinogenesis. We further analyzed the correlations between the methylation status of E-cadherin and E-cadherin protein expression and the clinicopathologic factors of HCCs.
MATERIALS AND METHODS
Tumor samples
Fresh samples of 64 HCCs and 13 DNs were obtained from 72 Korean patients at the Samsung Medical Center, Seoul, Korea, between 1999 and 2003. Informed consent was obtained from each patient included in this study. Twelve specimens were livers removed at orthotopic transplantation for HCC, and 60 were from curative surgical resections for HCC. None of the patients had received preoperative chemotherapy. Immediately after hepatectomy for primary HCC, fresh liver tissues were serially sliced at 4-5 mm intervals and then carefully examined by a pathologist for the presence of DNs and HCCs, which may be distinguished from the surrounding parenchyma by color, texture, or degree of bulging on the cut surface. Halves of the samples were snap-frozen in liquid nitrogen and stored at -80℃. The remaining halves were fixed in 10% neutral formalin to confirm the morphological diagnosis. DNs were histologically diagnosed according to the guidelines issued by the International Working Party (14), and HCCs were graded histologically according to the Edmondson and Steiner's criteria (16). Nontumorous livers showed cirrhosis in 58 patients and chronic hepatitis in 14. All patients were seropositive for hepatitis B surface antigen and had no serum antibody against hepatitis C virus. Patients ages ranged from 26 to 66 yr, with a median of 49.9 yr. The male-to-female ratio was 57:15. DNs ranged from 10 to 22 mm in longest diameter, with a median of 16.3 mm. There were 7 cases of low grade DN and 6 cases of high grade DN. The longest diameters of HCCs ranged from 11 to 140 mm, with a median of 45.8 mm. There were 13 cases of Edmondson & Steiner grade I, 39 grade II, and 12 grade III HCC. The histopathologic features of HCCs examined were tumor capsule formation, major portal vein invasion, microvascular invasion, tumor stage, tumor size, and histological differentiation. Microvascular invasion was considered as present when at least one or more endothelial cells or the tunica media of a vessel were observed to surround a neoplastic cell group. Tumor stage was determined according to the AJCC cancer staging criteria (17).
Immunohistochemistry
Formalin-fixed, paraffin-embedded tissues including both HCC or DN and adjacent nontumorous tissue were sectioned with 4 µm thickness. Immunohistochemical studies were performed using the streptavidin-biotin complex method and a TechMate™ 1000 automated staining system (DakoChemmate, Glostrup, Denmark). Primary monoclonal antibody against E-cadherin (clone 4A2C7) was purchased from Zymed Lab Inc. (San Francisco, CA, U.S.A.) and used at 1:40 dilution. Deparaffinized sections were treated with 3% hydrogen peroxide in methanol for 10 min to block endogenous peroxidase. Sections were processed in 0.05 M citrate buffer (pH 6.0) and heated in a microwave oven for 10 min for antigen retrieval. Sections were then incubated with the primary antibody for 60 min at 37℃. 3,3'-diaminobenzidine tetrahydrochloride was used as a chromogen, and Mayer's hematoxylin counterstain was applied. Negative controls were run simultaneously with an omission of primary antibody. Blocks of normal liver tissues were prepared as controls from the normal liver tissues of five patients with metastatic colonic carcinoma of the liver.
Strong intercellular and contiguous membranous staining was considered positive for E-cadherin expression. Staining results were evaluated by two independent pathologists and any interpretational differences were resolved by consensus. In accordance with previously published criteria (7), tumors were considered maintained immunoreactivity for E-cadherin when ≥50% of tumor cells showed strong membranous staining, and reduced immunoreactivity when >50% of tumor cells lacked or showed only slight membranous staining.
Methylation-specific PCR (MSP)
DNA methylation patterns in the E-cadherin promoter region were determined by MSP. Genomic DNA was obtained from fresh HCC or DN. DNA (1 µg) in a volume of 50 µL was denatured using NaOH (final concentration, 0.2 M) for 10 min at 37℃. Thirty µL of 10 mM hydroquinone and 520 µL of 3 M sodium bisulfite (pH 5), both freshly prepared, were then added and mixed, and samples were incubated under mineral oil at 50℃ for 16 hr. Modified DNA was purified using the Wizard DNA purification resin according to the manufacturer's instructions and then eluted into 50 µL of water. Modification was completed by treating with NaOH (final concentration, 0.3 M) for 5 min at room temperature, followed by ethanol precipitation. DNA was resuspended in water and either used immediately or stored at -20℃.
Bisulfite-modified DNA was amplified using methylated-specific primers (E-cad-M) 5'-TTAGGTTAGAGGGTTATCGCGT (sense) and 5'-TAACTAAAAATTCACCTACCGAC (antisense) or unmethylated-specific primers (E-cad-U) 5'-TAATTTTAGGTTAGAGGGTTATTGT (sense) and 5'-CACAACCAATCAACAACACA (antisense), which were designed for the E-cadherin promoter region by Herman et al. (18). These primers contained six sites (116 bp) of the CpG promoter at genomic position of -205 for E-cad-M and five sites (97 bp) at genomic position of -201 for E-cad-U, respectively (18). The PCR mixture contained 1× PCR buffer (16.6 mM ammonium sulfate/67 mM Tris, pH 8.8/6.7 mM MgCl2/10 mM 2-mercaptoethanol), dNTPs (each at 1.25 mM), primers (300 ng of each per reaction), and bisulfite-modified DNA (50 ng) in a final volume of 50 µL. PCR conditions were as follows: 95℃ for 5 min before adding 1.25 units of Taq polymerase; then 33 cycles of 95℃ for 30 sec, 57℃ for 30 sec for methylated-specific primers or 53℃ for 30 sec for unmethylated-specific primers, 72℃ for 30 sec; and finally 4 min at 72℃. Controls without DNA were performed for each PCR set. The product of each PCR (10 µL) was loaded directly into nondenaturing 6-8% polyacrylamide gels, stained with ethidium bromide, and visualized directly under UV illumination.
Statistical analysis
The chi-square test was used, and significance was accepted at p<0.05. Survival curves were plotted using the Kaplan-Meier method to assess the correlations between the various factors and survival. Differences between survival curves were estimated using the log-rank test. P-values <0.05 were considered significant.
RESULTS
E-cadherin expression
Diffuse strong membranous staining of E-cadherin was detected in the hepatocytes in the 5 normal liver tissues. Most areas of hepatocytes in nontumorous cirrhotic or chronic hepatitic liver tissues showed diffuse strong membranous staining of E-cadherin. Intrahepatic bile ducts showed strong and homogeneous membranous staining and thus served as an internal standard of positive staining.
Maintained immunoreactivity for E-cadherin was observed in all 13 DNs (100%) and 46 of the 64 (72%) HCCs. Reduced E-cadherin immunoreactivity was found in 18 of 64 (28%) HCCs:1 of 13 (7.7%) Edmondson and Steiner grade I, 12 of 39 (30.8%) grade II, and 5 of 12 (41.7%) grade III HCCs (Fig. 1). Reduced E-cadherin immunoreactivity was not correlated with tumor capsule formation, major portal vein invasion, microvascular invasion, tumor recurrence, tumor stage, tumor size, or histological differentiation of HCCs.
Promoter methylation of E-cadherin
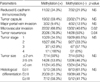
Methylation of the E-cadherin promoter region was detected in 1 high grade DN and 32 of 64 (50%) HCCs (Fig. 2). One of 13 (7.7%) DNs, 5 of 13 (38.5%) Edmondson and Steiner grade I HCCs, and 27 of 51 (52.9%) grade II or III HCCs were positive for methylation, showing a significant correlation between the methylation status and the stepwise progression of hepatocarcinogenesis (p=0.004). Reduced E-cadherin immunoreactivity was found in 11 of 32 (34.3%) HCCs with promoter methylation of E-cadherin and in 7 of 32 (21.9%) HCCs without promoter methylation. Methylation status was found to be significantly correlated with microvascular invasion (p=0.02) and tumor recurrence in HCCs (p=0.04), but methylation status was not correlated with reduced E-cadherin immunoreactivity, tumor capsule formation, or major portal vein invasion in HCCs. Methylation frequencies were not found to be correlated with the tumor stage, tumor size, or histological differentiation of HCCs (Table 1).
Survival analysis
After curative resection for HCC, 54 patients were followed up at our outpatient clinic and received regular clinical assessments to detect tumor recurrence. A diagnosis of recurrence was based on an elevated serum α-fetoprotein level and radiological evidence and/or biopsy. During the follow-up period (median, 43 months; range, 22-53 months), 34 patients experienced tumor recurrence and 24 patients died of the disease. Tumors recurred in residual livers in all 34 cases.
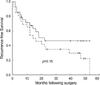
Median survival time for the 54 patients was 51 months and their median recurrence-free survival time was 18 months. Median recurrence-free survival time was 22 months in methylation-negative cases (n=29) and 14 months in methylation-positive cases (n=26). The Kaplan-Meier method showed that methylation status did not have a significant influence on the overall survival (p=0.91) or the recurrence-free survival of the 54 HCC patients (p=0.15; Fig. 3).
DISCUSSION
Work over the past several years has demonstrated that the silencing of tumor suppressor genes associated with promoter methylation is a common feature in human cancers, and that this serves as an alternative mechanism of loss of tumor suppressor gene function (11). A growing number of genes have been found to undergo promoter methylation in HCC, which indicates the potential role of promoter methylation in hepatocarcinogenesis. The down-regulation of E-cadherin is related to allelic deletion of the gene or DNA hypermethylation in the promoter region; both mechanisms have been demonstrated in HCC (13, 19). Reduced expression of E-cadherin decreases intercellular adhesiveness, and may result in the initiation of invasion and in the destruction of normal tissue morphology (7). The reported frequency of E-cadherin promoter methylation by MSP ranges from 33% to 49% in HCCs (15, 20), though it is significantly lower in one study (8.9%) (13). In the present study, we found a 50% frequency of E-cadherin promoter methylation in HCC, which demonstrates that it is a relatively frequent event. Kanai et al. (9) reported no significant differences in the incidences of aberrant DNA methylation on chromosome 16 between HCCs with hepatitis B or hepatitis C virus infection and HCCs without either.
DNs are precancerous lesions with a high risk of progression into HCCs. Lee et al. (15) detected the methylation of the E-cadherin CpG island in 33.3% of HCCs, but did not detect this methylation in all 22 DNs studied. In the present study, E-cadherin was found to be methylated in DNs at a frequency of 7.7% and methylation frequencies increased significantly to 38.5% in grade I HCCs and 52.9% in grade II or III HCCs. These results indicate that the increased frequency of E-cadherin promoter methylation appears to be associated with a more advanced stages of hepatocarcinogenesis, and suggest that E-cadherin methylation might participate in the stepwise progression of hepatocarcinogenesis. Some steps of carcinogenesis involving non-mutational genetic alterations may be reversible, thus aberrant DNA methylation might become a target for cancer prevention and therapy.
Recurrence after the successful surgical or nonsurgical treatment of HCC is caused either by intrahepatic metastasis or by metachronously multicentric occurrences. Intrahepatic metastasis is a major cause of recurrence of advanced HCCs with varying degrees of vascular invasion, and multicentric occurrence is a frequent cause of recurrence in small HCCs with no obvious vascular invasion. The inactivation of E-cadherin is involved in tumor invasiveness and metastatic potential (1). Moreover, promoter CpG island methylation is an important mechanism of gene inactivation in human cancer. In this study, we observed that promoter methylation of E-cadherin was significantly correlated with microvascular invasion and tumor recurrence. Promoter methylation of E-cadherin may participate in certain steps of hepatocarcinogenesis by reducing intercellular adhesiveness, which may result in invasion and metastasis. In this study, reduced E-cadherin immunoreactivity was not correlated with HCC recurrence. These data are in agreement with a previous report (13), and might reflect a high percentage of de novo onset of primary tumors over truly relapsed HCCs. No significant correlation was observed between reduced E-cadherin immunoreactivity and microvascular invasion in HCC. This is at variance with a previous report (13). The relation between reduced E-cadherin immunoreactivity and histopathologic features of HCCs needs further study.
Lee et al. (15) reported that HCC patients with E-cadherin methylation showed poorer overall survival than those without. However, in the present study, no significant correlation was observed between the methylation status of HCC and survival. A recent study found that the methylation status of E-cadherin promoter changed dynamically according to the cellular microenvironment in the tumor (21). MSP is a remarkably sensitive method that can detect 0.1% of methylated cells in a specimen (18), and methylation status on an all-or-nothing basis may not directly predict the prognosis. Thus the extent of methylated areas within a single tumor may be more relevant to survival of HCC patients.
Kanai et al. (7) reported a significant correlation between CpG methylation around the promoter region and reduced E-cadherin expression in HCCs. However, in the present study, no significant correlation was found between the methylation status of HCC and E-cadherin immunoreactivity, which is consistent with previous reports (6, 13). Promoter methylation of E-cadherin was heterogeneous among cells in single HCCs (19). Moreover, intratumoral E-cadherin expression heterogeneity was noted in human cancers (22). Graff et al (21) reported that breast cancers with minimal evidence of E-cadherin methylation displayed generally strong E-cadherin immunoreactivity, whereas those with prominent methylation showed distinct, heterogeneous loss of E-cadherin immunoreactivity. Methylation status on an all-or-nothing basis may not directly predict the E-cadherin immunoreactivity, and the extent of methylated areas within a single tumor may be more relevant to the E-cadherin immunoreactivity. In addition, we noted reduced E-cadherin immunoreactivity without methylation in 21.9% of HCCs. This suggests that mechanisms other than methylation are likely to be involved in impaired E-cadherin immunoreactivity. Dysfunction of catenins or the effects of signals from other cell junctions might induce the instability of translated E-cadherin molecules.
In conclusion, the methylation of the E-cadherin promoter region was found to be a frequent event in HCC, and may play an important role in the stepwise progression of hepatocarcinogenesis. Moreover, the promoter methylation of E-cadherin in HCC was found to be significantly correlated with microvascular invasion and recurrence.


 XML Download
XML Download