

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Previous randomized studies have demonstrated that coronary artery bypass grafting (CABG) was associated with fewer episodes of angina, less requirement for repeated revascularization, but similar rates of death or myocardial infarction (MI) compared with percutaneous coronary intervention (PCI) (1-7). The Bypass Angioplasty Revascularization Investigation (BARI) study reported a better long-term survival rate in the CABG group for diabetic patients (8). However, those studies were performed in the pre-stent era and are therefore not representative of currently available technologies. The use of stents for percutaneous coronary artery intervention decreases acute complications, late restenosis, and the requirement for repeated revascularization (9, 10). Recently, an Argentinian randomized study showed that percutaneous coronary stent implantation was superior to CABG in terms of both survival and MI (11). However, recent American and European trials reported that CABG was associated with a similar survival rate and stroke- or MI-free survival as PCI (12, 13). Many studies are underway to clarify this issue. In Asia, however, studies comparing CABG and PCI are rare.
The Korean Multicenter Revascularization Registry (KORR) is a retrospective registry with physician-guided selection of treatment. This study was designed to assess the relative merits of PCI versus CABG in the post-stent era in multivessel coronary artery disease (MVCAD), particularly for diabetic patients.
MATERIALS AND METHODS
Study design
This study is in compliance with human studies committees in our hospital and Food and Drug Administration guidelines. For the study was designed as a retrospective registry of PCI and CABG, the distribution of baseline characteristics was not comparable between the two groups. We adjusted the distribution of several risk factors that were found to be important for clinical events, as described below.
Screening process
Patients with two- or three-vessel coronary artery disease who underwent elective PCI or CABG between January 1995 and December 2000 in one of nine centers in Korea were enrolled in this registry. Patients with stable angina, acute coronary syndrome (ACS), acute myocardial infarction (AMI), or silent myocardial ischemia were included. Patients with cardiogenic shock, AMI indicated for primary PCI, concomitant valve surgery, a history of CABG, or mechanical complications such as ventricular septal defect, myocardial free-wall rupture, or mitral regurgitation, were excluded. Patients with significant left main disease were also excluded, to reduce the disparity in disease severity between the CABG and PCI groups. A total of 3,279 patients were included: 1,182 treated with CABG and 2,097 with PCI.
CABG and PCI techniques
CABG was performed with standard surgical techniques. Complete revascularization was attempted whenever possible, using arterial conduit or saphenous vein grafts. PCI was also performed using standard techniques. Patients were treated with aspirin (100-300 mg daily) 24 hr before the procedure. Ticlopidine (500 mg daily) or cilostazol (500 mg daily) was given when stent implantation was planned, and continued for at least two weeks after stent implantation. Intravenous heparin was used to maintain an activated clotting time of more than 300 sec during the procedure. The use of abciximab was limited to 0.8%. Stents were used for either bail-out or elective procedures.
Adjustment of disparities in the distribution of prognostic factors
Compared to CABG group, PCI group showed significantly higher proportion of patients with old age (age≥65 yr), clinical diagnosis of AMI, normal left ventricular function. The clinical diagnosis of ACS, treated diabetes (diabetes currently treated with oral hypoglycemic drugs or insulin), and history of smoking, previous PCI, and previous cerebrovascular event (CVE) history were significantly less frequent in PCI group, respectively. Coronary angiogram showed significantly lower proportion of 3-vessel disease and proximal LAD lesion in PCI group, too. Risk factors for major adverse cardiac events (MACE) with the corresponding odds ratios are listed in Table 1. MACE was defined as death, myocardial infarction (MI), revascularization, or CVE.
Statistical adjustments were required to control for disparities in the distribution of independent prognostic factors between the PCI and CABG groups. Matched variables included old age (age≥65 yr), clinical diagnosis (ACS or AMI), normal left ventricular function, CVE history, and the presence of a significant lesion in the proximal left anterior descending artery. The presence of diabetes was not matched because we intended to evaluate the impact of diabetes on clinical outcome, according to the two treatment modalities. A total of 2,154 patients were selected for the statistically adjusted population. The clinical and angiographic characteristics of the selected patients are listed in Table 2. CABG and PCI groups were compared for the matched population.
Statistical analysis
Results are presented as means±standard errors of the means. A χ2 test was used to determine the significant differences in categorical variables. For comparison of continuous variables, an unpaired t-test was used. For continuous variables with a distribution other than a normal distribution, a Wilcoxon two-sample test was used. Multivariate logistic regression analysis was performed to identify independent prognostic factors. A log-rank test was used for the comparison of Kaplan-Meier survival curves between groups. All tests were two-tailed, and a p-value ≤0.05 was considered to be statistically significant.
RESULTS
Overall results
The average follow-up period was 2.1±1.6 yr (range, 0-6.6 yr). Eighty-four per cent of patients were followed-up for more than one year, and 47.1% for more than three years.
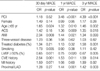
There was no significant difference between the short- and long-term mortality rates in the PCI and CABG groups up to three years. The long-term incidence of morbidity (death, MI, or CVE) was also not significantly different between groups, but the 30-day incidence was significantly higher in the CABG group (CABG 4.0%, PCI 1.3%, p=0.001), which was mainly due to a higher incidence of CVE in the CABG group (CABG 2.8%, PCI 0.1%, p<0.001; Table 3, Fig. 1). However, the incidence of MACE (death, MI, CVE, or revascularization) was significantly higher in the PCI group than in CABG group after one year, which was due to a higher incidence of revascularization in the PCI group.
Influence of diabetes on clinical outcome
Of the matched population, 693 patients (32.2%) had a history of diabetes and 566 patients (26.3%) were being treated with oral hypoglycemics or insulin (treated diabetic patients) at the time of revascularization. In non-treated diabetics, 83.7% of patients were followed-up for more than a year, and 47.9% for more than 3 yr, and in treated diabetics, 83.0% for more than a year and 44.9% for more than 3 yr.
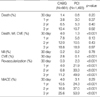
Mortality rates were similar between the CABG and PCI groups, for both the treated and non-treated diabetic patients (Table 4, Fig. 2). In treated diabetic patients, the 30-day mortality rate was 2.22-fold higher, whereas the three-year mortality rate was 1.92-fold lower in the CABG group, although these differences were not statistically significant. In none-treated diabetic patients, however, the odds ratio was virtually not changed over three years. Treated diabetes was associated with higher three-year mortality only in the PCI group (non-treated diabetes 8.3%, treated diabetes 19.8%, odds ratio=2.74, p=0.002).
The 30-day incidence of morbidity (death, MI, or CVE) in the CABG group was significantly higher than in the PCI group, for both non-treated and treated diabetics (non-treated diabetics: CABG 3.3%, PCI 1.0%, p=0.002; treated diabetics: CABG 5.6%, PCI 2.0%, p=0.026), mainly due to a higher incidence of CVE in the CABG group. The 30-day incidence of CVE was significantly higher in both non-treated and treated diabetics (non-treated diabetics: CABG 2.4%, PCI 0.1%, p<0.001; treated diabetics: CABG 3.6%, PCI 0.0%, p<0.001).
CABG was preferable to PCI in terms of the risk of revascularization, for both non-treated and treated diabetic patients. Treated diabetes was a significant prognostic factor for three-year revascularization (non-treated diabetes 46.9%, treated diabetes 60.5%, odds ratio=1.29, p=0.003) and three-year MACE rate only in the PCI group (non-treated diabetes 50.9%, treated diabetes 62.2%, odds ratio=1.26, p=0.002). However, in CABG group, treated diabetes was not a significant risk factor for any event.
MACE in diabetic subgroups within and between treatment cohorts
None of the mortality, morbidity, or MACE rates differed significantly among the four diabetes treatment modality groups, either in the CABG or PCI groups (Fig. 3). Insulin-treated diabetic patients, however, had a higher risk of MACE than non-diabetic patients in the PCI group (p=0.038).
Arterial graft vs. stent
Stents were used in 68.5% of PCIs. Stent implantation was associated with reduced 1-yr death or MI risk (non-stent 7.1 %, stent 3.6%, p=0.014) and reduced 30-day revascularization rate (non-stent 3.6%, stent 1.6%, p=0.02). Arterial graft was performed in 92.1% CABGs. The left internal mammary artery was used in 91.1% of cases. In 14.2% of CABGs, only arterial grafts were used. In 23.0% of CABGs, surgical procedures were performed without a cardiopulmonary bypass pump. The arterial graft group showed a significantly lower three-year mortality rate (arterial graft 8.6%, vein graft 21.6 %, p=0.016) and a lower three-year MACE rate (arterial graft 23.2%, vein graft 40.5%, p=0.017) compared with the veingraft-only group.
To compare current therapeutic technologies, the rate of MACE was compared between the stent and arterial graft groups. Thirty-day revascularization was reduced in the stent group and did not differ significantly from that of the CABG-with-arterial-graft group. Otherwise, the results were similar to those of the total adjusted population.
DISCUSSION
This study is the first Korean multicenter registry that compares the long-term clinical outcomes of two currently used coronary revascularization strategies. Short- and long-term mortality rates did not differ significantly between the PCI and CABG groups after up to three years of follow-up. Early morbidity was higher in the CABG group than in the PCI group, due to a higher rate of CVE. Three-year event-free survival was much higher in the CABG group than in the PCI group, due to an increased rate of revascularization in the PCI group.
Short- and long-term mortality rates did not differ significantly between the PCI and CABG groups for diabetic or non-diabetic patients, although there was a trend in the PCI group towards an increased three-year mortality rate among diabetics. In the PCI group, diabetes was associated with significantly higher mortality and MACE rates at three years, in contrast to the CABG group in which the two cohorts did not differ. In a separate analysis of arterial graft vs. stent, the short- and long-term outcomes were similar to those of the total adjusted population.
Our current practice of selecting the treatment modality for patients with MVCAD is based on the results of many prior randomized trials (1-7). The BARI study is representative of the pre-stent era. It demonstrated that CABG was more successful than PCI in terms of the seven-year survival rate, mainly due to the beneficial effects of CABG for diabetic patients. The seven-year survival rate was 65.5% for PCI and 80.6% for CABG in the diabetic group (p=0.003) (8). In non-diabetics, there was no difference in survival after PCI or CABG. In the Emory Angioplasty versus Surgery Trial (EAST), treated diabetics showed similar mortality rates to non-treated diabetics until the three-year follow-up. However, the curves began to diverge after five years, and by eight years, mortality rates were better after surgery, although the differences were not statistically significant (14). The Northern New England Cardiovascular Disease Study also showed that diabetics treated with PCI had mortality rates significantly higher than patients undergoing CABG (hazard ratio=1.49, p=0.037) (15). Mortality risk tended to increase more among patients with three-vessel disease (hazard ratio=2.02, p=0.038) than among patients with two-vessel disease (hazard ratio=1.33, p=0.21).
In contrast, the BARI registry showed that seven-year survival was similar after PTCA or CABG (85.8% for PCI, 86.1% for CABG, p=0.66) (16). Even among diabetics, PTCA and CABG showed similar seven-year survival rates (74.0% for PCI, 74.0% for CABG). The results of the Coronary Angioplasty versus Bypass Revascularization Investigation (CABRI) trial also indicated that there was no significant difference in four-year mortality rates between patients randomized to either PCI or CABG strategies, in either diabetic or non-diabetic patients, although diabetes was a significant risk factor for mortality (17). Duke University database also noted similar long-term outcomes after either PCI or CABG for diabetic patients with multivessel disease (18).
Since the completion of these early major trials, significant technological advances have been made in the field of coronary revascularization, in both PCI and CABG. Stent implantation is associated with greater clinical success, and a significantly lower long-term revascularization rate (9, 10). Recent PCI vs. CABG studies in the management of MVCAD have utilized advanced technologies including stent implantation. The Argentine randomized study (ERACI-II) also showed a better survival rate with PCI than with CABG after 30 days and at one year (11). However, the Arterial Revascularization therapies Study (ARTS) and the Angina With Extremely Serious Operative Mortality Evaluation (AWESOME) study demonstrated similar mortality rates after 2-3 yr for PCI and CABG (12, 13). Repeat revascularization rates seemed to improve in the stent group compared with the rates for the balloon groups of previous studies. However, rates of revascularization were still significantly higher than those of the CABG group, particularly for treated diabetics.
The prevalence of diabetes has been increasing explosively in Korea, as in other eastern societies (19). This is also true for mortality from coronary artery disease, which parallels the prevalence of diabetes (20). Treatment for coronary artery disease in diabetic patients is still not satisfactory in terms of long-term mortality and morbidity. Despite many multicenter trials, the most appropriate selection of a revascularization strategy remains to be established, particularly in diabetic patients with multivessel disease. Moreover, in Asian countries, studies comparing long-term outcomes of PCI and CABG in patients with advanced coronary artery disease are rare.
In Korea, Sim et al. reported similar early clinical outcome and higher long-term target lesion revascularization rate in the coronary stent group compared to coronary artery bypass group in single center registry of 160 patients (30.5 months follow-up: stent group 18.9%, bypass group 5.7%, p<0.005) (21). This Korean registry study will increase our understanding of the current situation and the outcomes associated with revascularization procedures in this region of the world.
KORR showed similar short- and long-term mortality rates for the two therapeutic modalities. These results are consistent with most previous comparative studies on PCI vs. CABG in the management of MVCAD. Similar survival rates were observed for both diabetic and non-diabetic patients. This finding is at variance with the BARI trial, but is similar to the results of the ARTS (22) and BARI registry. In the ERACI II study, the 30-day mortality rate was significantly higher in the CABG group than in the PCI group, due to the high mortality in the CABG group (PCI 0.9%, CABG 5.7%, p=0.013), which is partly attributable to the high proportion of patients with ACS in this study (11). In our data, however, the 30-day mortality rate of patients with ACS was less than 2.0% in both revascularization groups (CABG 1.1%, PCI 0.3%, p=0.081).
Our data indicate that the early morbidity rate may be higher in the CABG group than in the PCI group. In the ARTS, the risk of MI or CVE was similar in the two groups (13). However, in KORR, the 30-day CVE risk was significantly lower in the PCI group. The incidence of CVE in KORR was lower than in the ARTS (KORR stent group, 30 days CVE, 0.0%, and one-year CVE, 0.6%; ARTS, one-year CVE, 1.5%). The rate of CVE in this study was similar to that of the PCI group in the ERACI II trial (30 days CVE, 0.0%) (11). Although the repeat revascularization rate after PCI was higher than after CABG, the rate difference between diabetics and non-diabetics in KORR was less pronounced than in the ARTS study.
When considering the relative merits of the two revascularization techniques in the management of MVCAD in the post-stent era, the two techniques seem equivalent in terms of survival. However, CABG appears to be superior to PCI insofar as the requirements for repeat revascularization is lower.
Treated diabetes was a risk factor for long-term mortality only in the PCI group, but the relative advantages and disadvantages of CABG compared with PCI did not differ markedly between diabetic and non-diabetic patients in this study. The survival benefit of CABG over PCI for diabetic patients has been demonstrated only in studies with longer-term follow-ups than that used in this study. The follow-up period was less than three years in several recent studies, including ERACI II, ARTS, and AWESOME. In the EAST trial, the benefits of CABG for diabetics were demonstrated only after five years. The survival curves for diabetic patients of this study began to diverge after two years and showed a mortality rate in the PCI group almost twofold higher than that of the CABG group, although the difference was not statistically significant.
A common problem of long-term comparative studies of PCI vs. CABG is that the results may become obsolete even before publication, due to the speed of technological development and advancement. Recently, drug-eluting stents have shown very promising results on restenosis (23, 24). The restenosis rate following stenting may be lowered further in the future. Therefore, PCI with drug-coated stents may achieve similar or even better outcomes than those of CABG, and comparative assessments of drug-coated stent versus CABG may be necessary in the near future.
One of the limitations of this study is that KORR is a retrospective and non-randomized study with physician-guided selection of treatment. Although the differences measured between the two treatment groups were controlled, this statistical adjustment can be imperfect. Another important limitation is that the long-term follow-up rate is relatively low compared to previous western studies. Therefore, the two- or three-year event rate may be even less reliable. The third limitation is that the stent implantation rate was only 68.5%, which is relatively low considering current practice of PCI in Korea, because the patients of this study had been recruited before year 2001. Moreover, drug-eluting stents have been already on the market for more than a year and dramatically changed the revascularization strategy in the patients with multi-vessel disease. The difficulty in keeping up the current practice pattern always has been one of the major limitations of large trials or registries with long term follow-up. The contemporary techniques should be considered to interpret and apply this data to current practice in Korea.
As a conclusion, in this multicenter Korean registry, we found that survival rates were similar after PCI and CABG for treated diabetics as well as for the total population. Compared with CABG, PCI was associated with a lower incidence of short-term morbidity but with a greater requirement for repeated revascularization, particularly in treated diabetics.





 XML Download
XML Download