

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Polymyositis (PM) is an autoimmune inflammatory myopathy characterized by chronic inflammation of skeletal muscle with infiltration of lymphocytes. Although controversy still remains concerning the relationship between malignancy and myositis, most authorities agree that there is an increased incidence of malignancy in myositis patients, especially in the case of dermatomyositis (DM). For PM, however, the evidences which favor the association with malignacy is not sufficient than DM (1). This consideration is, partly, because of the interval between the time of cancer diagnosis and the time of myositis development. Zantos et al. found that the risk of cancer was increased in 1-5 yr after myositis in most cases of PM, in contrast to 4 yr prior through 4 yr after the myositis diagnosis in DM (2).
Paraneoplastic syndromes including erythrocytosis, hypoglycemia, hypercholesterolemia and porphyria cutanea tarda are reported in patients with hepatocellular carcinima (HCC), however, a few cases of PM associated with HCC have been reported (3-6).
Skeletal muscle injuries without trauma including metabolic myopathy, certain drugs and toxins, infections, electrolyte imbalances, and endocrine disorders may cause rhabdomyolysis. Rhabdomyolysis is one of the leading causes of acute renal failure (ARF). Inflammatory myopathies including PM also rarely result in myoglobinuric ARF. There have been a few reported cases of PM with rhabdomyolysis leading to ARF requiring hemodialysis (7-10). Here we describe a case with HCC associated with PM presenting as fulminant rhabdomyolysis and ARF.
CASE REPORT
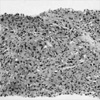
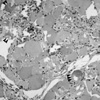
A 55-yr-old man was admitted to our hospital because of oliguria and progressive proximal muscle weakness of the lower limbs. Two weeks earlier, prior to admission into the hospital, he felt fine. He began experiencing chill, malaise and myalgia. The patient complained of right upper quadrant abdominal pain. Past medical history was not contributory. The patient denied ethanol ingestion and recent use of drugs. He also denied any traumatic injury. On physical examination, he looked acutely ill. Temperature was 36.7℃, respiration rate 24/min, and blood pressure 110/70 mmHg. Auscultation of the heart and both lungs were normal. The abdomen was soft. The edge of the liver descended 3 cm below the right costal margin. Proximal muscle weakness was marked and muscle power was grade 3 for the lower limbs and grade 4 for the upper limbs. The laboratory investigations were as follows: WBC count 12,700/µL (segmented neutrophil 81%), hemoglobin 13.9 g/dL, platelet 189,000/µL, total protein 6.8 g/dL, albumin 3.0 g/dL, AST 1,074 U/L, ALT 764 U/L, alkaline phosphatase 82 IU/L, GGT 38 U/L, total bilirubin 1.0 mg/dL, international normalized ratio for prothrombin 1.6, BUN 99 mg/dL, creatinine 9.1 mg/dL, calcium 6 mg/dL, phosphorus 7.6 mg/dL, ionized calcium 0.7 mmol/L (normal 1.05-1.35 mmol/L), intact parathyroid hormone 201.87 pg/mL (normal 12-72 pg/mL). erythrocyte sedimentation rate 55 mm/hr, C-reactive protein 200 mg/dL, creatine kinase 40,000 U/L, LDH 3,286 U/L, serum aldolase 66 sigma U/mL, serum myoglobin 1,140 ng/mL, and urine myoglobin 948 ng/mL. Urinalysis revealed 10-20 RBC per high power field. Urine myoglobin was positive and urine hemoglobin was negative. Tests for anti-HBs, anti-HCV, anti-HAV, anti-HIV, rheumatoid factor, anti-nuclear antibody, anti-dsDNA antibody, anti-neutrophil cytoplasmic antibody, anti-Jo-1 antibody were all negative. Serum levels of complements and alpha-fetoprotein were normal. Hypercalcemia appeared on day 14 and lasted for 28 days. The serum level of intact PTH measured on the 37th hospital day was 5.81 pg/mL. A chest radiograph showed bilateral pleural effusion. Computed tomography of the abdomen demonstrated a 6 cm sized-exophytic bulging mass in the hepatic angle. Two smaller satellite nodules near the main hepatic mass and several enlarged intraperitoneal lymph nodes were also detected. A radionuclear bone scan image showed increased uptake of radioisotope in the most of the skeletal muscles including the both lower limbs, indicative of inflammatory myopathy or rhabdomyolysis. Fat suppressed T2-weighted MR imaging of the thigh showed high signal intensity and gadolinium enhancement along the whole length of vastus muscle group, biceps femoralis and adductor longus. Needle electromyography showed spontaneous activity of fibrillations, sharp positive waves, polyphasic motor unit potentials of low amplitude, and short duration in all muscle fibers during voluntary contraction. The muscle biopsy was obtained from the left thigh and showed extensive myofiber necrosis with heavy infiltration of macrophages within necrotic fibers, multifocal calcifications in myofibers, and multifocal lymphocytic infiltrations in endomysium (Fig. 1). The emergent hemodialysis was initiated with a tentative diagnosis of ARF. After 15 days with hemodialytic support, his renal function was gradually restored to allow withdrawal of dialysis. The liver biopsy was performed on the 20th day of hospitalization under ultrasonographic guidance. Immunohistochemical stain of biopsied tissue showed positive for AFP and negative for CEA, and poorly differentiated HCC was diagnosed (Fig. 2). Under the diagnosis of PM, our patient was put on methylprednisolone (1 mg/kg/day) concurrently with hemodialysis. Treatment was switched to oral prednisolone and persisted for following 5 weeks. However, muscle power did not improve significantly. Chemotherapy for HCC was considered, but the patient had an episode of hemorrhagic shock from a sudden rupture of hepatic mass on the 44th day of hospitalization. He progressively deteriorated and remained in an unstable condition until he passed away on the 54th day.
DISCUSSION
On the matter about the association of malignancy and myositis, major excess risk was attributable to DM. PM is generally considered that there is much weaker relation with malignancy than DM. However, we concluded that it is more reasonable to diagnose for our patient as PM based on the followings. First of all, our patient presented no apparent skin lesion for DM. Typical skin lesions are essential components for diagnosing the DM. Second, DM has been too rarely associated with HCC compared of its epidemic, particularly in Korea.
Myoglobinemic ARF could be caused by non-traumatic skeletal muscle injury. Up to now, less than ten cases of the PM-induced myoglobinemic ARF have been reported in the literature. PM/DM could be presented as one of paraneoplastic manifestations, but only some cases of HCC-associated with PM/DM have been reported. This is a rare reported case of PM associated with HCC, present with fulminant rhabdomyolysis and ARF. Because of the rapidly deteriorating condition of the patient, it is difficult to determine whether PM occurred as a paraneoplastic syndrome or took place coincidentally with HCC in our case. A causal relationship between HCC and PM/DM was demonstrated in the case reported by Hasegawa et al. (3). Although the pathogenesis of PM/DM has not been clarified, two reports suggested that HCV-induced autoantibodies or circulating immune complexes could contribute to the pathogenesis of PM/DM (11, 12). Hepatitis C virus was not detected in our case. Myoglobinuria occurs not infrequently in patients with PM/DM, but it is rarely followed by ARF. About the pathophysiology of renal failure in rhabdomyolysis, Lewington et al. documented acute tubular necrosis and obstructive tubular cast of myoglobin in renal biopsy from the case of ARF which was attributed to rhabdomyolysis, secondary to PM (8).
Both early hypocalcemic and late hypercalcemic phase were observed in this case. Either hyperphosphatemia-induced bone resistance to PTH or decreased levels of 1,25 dihydroxyvitamin D have been implicated as precipitating factors in the development of hypocalcemia. In the case of massive muscle necrosis and extensive calcification, the movement of calcium into necrotic muscle is regarded as a major contributory factor. Remobilization of calcium from muscles has been thought to be a main mechanism for the development of subsequent hypercalcemia (13).
Massive muscle calcification in ARF caused by non-traumatic rhabdomyolysis has been rarely reported, whose mechanism has not been clarified yet. Coakley and colleagues (14) suggested that leakage of calcium into inflamed muscle cells where the phosphate concentration is high, leads to intracellular deposition of calcium phosphate. But Gray et al. (15) suggested that hyperphosphatemia, which is due to the release from damaged muscle cells, and the decreased renal clearance of phosphate are the main mechanisms for muscle calcification. Adams et al. (16) reported that muscle calcification could occasionally be seen, and appears as hypo-intense areas on MR imaging in patients with idiopathic inflammatory myopathies.
To our knowledge, this is the first reported case of PM in which massive muscle calcification is proven pathologically. Akmal et al. (17) demonstrated that calcium deposits in damaged muscles occur during the oliguric phase of ARF due to rhabdomyolysis, and the calcification disappears with recovery of renal failure. Unfortunately, we did not follow up on muscle calcification after recovery from oliguric phase of ARF. Our case demonstrates that PM could be associated with HCC and instigate rhabdomyolysis leading to ARF. PM must be considered in the differential diagnosis of non-traumatic rhabdomyolysis and investigation for the associated malignancy, including HCC, should be included.
 XML Download
XML Download