

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gabapentin is an antiepileptic agent that attenuates hyperalgesia in models of tissue injury pain without affecting acute noxious stimuli threshold (1, 2). The antinociceptive effect of gabapentin is more potent after intrathecal rather than systemic delivery (3). These findings suggest that gabapentin can alter the facilitated state which occurs secondary to the persistent afferent input generated by a local tissue injury and that the major site of action of gabapentin may be the spinal cord. Several receptors, including N-methyl D-aspartate (NMDA) receptors, have been suggested as the sites of action of gabapentin (4).
Adenosine is an endogenous purine compound with a modulatory effect on nociceptive information at the spinal level (5). Although intrathecal adenosine decreases the facilitated state (6-8), the effect for acute nociception is different according to tested stimuli (7-10). The antinociception of intrathecal adenosine is mediated through adenosine receptors in the dorsal horn of the spinal cord (11).
The above findings suggest that gabapentin and adenosine may exert their actions mainly on the facilitated state at the spinal level. However, the drug interaction between gabapentin and adenosine has not yet been determined.
Thus, the aim of the current study was to observe the effects of intrathecal gabapentin and adenosine on the formalin-evoked pain behavior and to determine the characteristics of their interaction at the spinal level.
MATERIALS AND METHODS
The Institutional Animal Care Committee of the Research Institute of Medical Science at Chonnam National University approved all experiments. Male Sprague-Dawley rats weighing 250-300 g were used. Rats were housed in group cages on a 12 hr night/day cycle with free access to food and water at all times. An intrathecal catheter was implanted during enflurane anesthesia previously described (12). Rats showing neurological deficits postoperatively were not used for subsequent experiments. Experiments started 4-5 days after intrathecal catheter insertion.
Drugs used in this study were as follows: gabapentin (1-[aminomethyl] cyclohexanacetic acid, Sigma Chemical Co., St., Louis, MO, U.S.A.), adenosine (Research Biochemical Internationals, Natick, MA, U.S.A.). Gabapentin and adenosine were dissolved in normal saline and dimethylsulfoxide (DMSO), respectively. Intrathecal administration of drugs was performed using a hand-driven, gear-operated syringe pump. All the drugs were delivered in a volume of 10 µL solution.
Pinna reflex, corneal reflex and motor function were examined after intrathecal administration of gabapentin (300 µg, n=5) and adenosine (300 µg, n=5). Motor function was assessed by the placing-stepping reflex and the righting reflex. The placing-stepping reflex was checked by drawing the dorsum of either hind paw across the edge of the table. Normal rats try to put the paw in front of the other when they walk. The righting reflex was evaluated by placing the rat horizontally with its back on the table. Normal rats give rise to an immediate and coordinated twisting of the body to an upright position. These behaviors were measured at 5, 10, 20, 30, 40, 50 and 60 min after intrathecal administration of gabapentin and adenosine, and judged as either present or absent.
The formalin test was performed as a nociceptive model. Subcutaneous injection of formalin solution (5%, 50 µL) into the plantar surface of the hindpaw with a 30 gauge needle produces the specific behavior of flinching/shaking of the affected paw. This formalin-induced behavior was regarded as a pain response and monitored for 60 min. The number of flinching/shaking response was counted for 1 min periods at 1-2 min and 5-6 min, and at 5 min intervals at 10-60 min. Two different phases were observed after formalin injection: phase 1, 0-9 min after formalin injection, and phase 2, 10-60 min after formalin injection.
On the experiment day, rats were randomly assigned to one of the drug treatment groups. The drug vehicles were used as a control (saline, n=7; DMSO, n=5). Rats received only one dose of drug or drug combination. The formalin test was carried out only once in the same rat.
For evaluation of the time course and dose-response of the antinociceptive action of gabapentin (10 µg, n=7; 30 µg, n=6; 100 µg, n=7; 300 µg, n=7) and adenosine (10 µg, n=6; 30 µg, n=6; 100 µg, n=9; 300 µg, n=7), both agents were intrathecally administered.
Intrathecal drugs were injected 10 min before formalin injection. Each ED50 value (effective dose producing a 50% reduction of control formalin response) of two agents was separately determined.
In order to determine the nature of the pharmacologic interaction between gabapentin and adenosine, an isobolographic analysis was used (13). Because both gabapentin and adenosine did not alter the phase 1 response, an isobolographic analysis was performed only during phase 2 of the formalin test. This method is based on comparisons of doses that are determined to be equi-effective. The ED50 values were calculated for each drug from the dose-response curves of the agents alone. Then, gabapentin and adenosine were administered concurrently at doses of the ED50 values (n=7) and fractions (1/2, n=6; 1/4, n=7; 1/8, n=8) of ED50 of each drug. The mixture was delivered 10 min before the formalin test. The ED50 values of the individual drugs given in combination were calculated from the dose-response curves of the combined drugs, and then these values were used for plotting the isobologram. The isobols were drawn by plotting the experimentally determined ED50 value of gabapentin on the X axis and that of adenosine on the Y axis delivered alone and in combination. The theoretical additive dose combination was calculated. From the variance of the total dose, individual variances for the agents in the combination were obtained. Furthermore, to describe the magnitude of the interaction, a total fraction value was calculated as follows.
Total fraction value = ED50 of drug 1 combined with drug 2/ED50 for drug 1 given alone + ED50 of drug 2 combined with drug 1/ED50 for drug 2 given alone
The fractional values indicate what portion of the single ED50 value was accounted for by the corresponding ED50 value for the combination. Values near 1 indicate an additive interaction, values greater than 1 imply an antagonistic interaction, and values less than 1 indicate a synergistic interaction.
Data are expressed as mean±SEM. The time response data are presented as the number of flinches. The dose-response data are presented as the sum of the number of flinches in each phase. To calculate the ED50 values of each drug, the number of flinches was converted to "percentage of control" as follows:

Dose-response data were analyzed by one-way analysis of variance with Scheffe for post hoc. The dose-response lines were fitted using least-squares linear regression, and ED50 and its 95% confidence intervals were calculated according to the previous method (14).
The difference between theoretical ED50 and experimental ED50 was examined by t-test. Differences were considered to be significant if p<0.05.
RESULTS
The total number of rats used in this study was 102 with 5-9 rats per group. Neither gabapentin nor adenosine affected pinna reflex, corneal reflex or motor tone after intrathecal administration.
Subcutaneous injection of formalin into the hindpaw resulted in a biphasic flinching response of the injected paw. Fig. 1 shows the time course of the effect of intrathecal gabapentin and adenosine, administered 10 min before formalin injection, in the formalin test.
The sum of the number of flinches in the saline or DMSO control group was not different from each other in phase 1 (22±2 vs. 18±1) or phase 2 (168±18 vs. 165±17). Intrathecal gabapentin and adenosine did not alter the flinching response during phase 1. During phase 2, both drugs produced a dose-dependent suppression of the flinching response (Fig. 2).
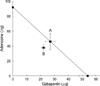
The phase 2 ED50 values of gabapentin and adenosine were 54 and 92 µg, respectively. Thus, the calculated dose ratio for gabapentin and adenosine was 0.59:1. Isobolographic analysis conducted in phase 2 revealed an additive interaction between gabapentin and adenosine. The experimental ED50 value did not differ from the theoretical ED50 value (Fig. 3). The ED50 value of the gabapentin in the mixture of gabapentin-adenosine was 60 µg. The total fraction value was 0.81, indicating an additive interaction (Table 1).
DISCUSSION
In the present study, intrathecal gabapentin and adenosine had little effect on phase 1 response in the formalin test. In contrast, these two drugs attenuated the phase 2 response. These observations suggest that spinal gabapentin and adenosine may alter the facilitated component of the response evoked by persistent afferent input with no effect on acute nociception.
The afferent input generated by formalin injection into the paw is believed to release excitatory amino acids, such as glutamate, which initiate a cascade through NMDA receptors (15). The resulting cascade is thought to cause the excitatory effect followed by a state of facilitation. Although the antinociceptive mechanisms of action of spinal gabapentin remain unclear, NMDA receptors seem to be relevant to the antinociception of gabapentin. The NMDA receptors exist in the substantia gelatinosa of the dorsal horn and are responsible for the spinal nociceptive processing (16-18). Recent studies have shown that gabapentin decreases glutamate concentrations and inhibits the release of glutamate and glutamatergic synaptic transmission presynatically (19-21). Furthermore, although there is no direct evidence of gabapentin binding to NMDA receptors, an agonist at the nonstrychnine site of NMDA receptors reversed the antinociceptive effect of gabapentin (4). These findings jointly suggest that spinal gabapentin may act on the NMDA receptors, attenuating the facilitated state. This antinociceptive effect of gabapentin is consistent with previous data (22, 23).
It has been acknowledged that adenosine may play an important role in the modulation of nociceptive inputs (5). Adenosine receptors have been identified in the substantia gelatinosa on intrinsic neurons (10). Thus, the antinociceptive action of adenosine may be mediated through spinal adenosine receptors. In this study, particularly, the effect of spinal adenosine for the facilitated state is in line with other reports (6-8). However, the effect for acute pain is consistently or differently noted. It has been reported that the phase 1 flinching response of the formalin test was not inhibited by an adenosine agonist in the spinal cord (6), but reversed by the other agonist (8). It has been demonstrated that intrathecal adenosine had little effect on the withdrawal latency to thermal stimulation (9), but increased the tail immersion latency (10). Although such discrepancy of adenosine for acute nociception has not been fully understood, it may be caused by the different types of tested stimuli and difference in drugs and dosages.
Isobolographic analysis of the current study showed an additive interaction between gabapentin and adenosine in the phase 2 response. These results indicate that gabapentin cannot potentiate the antinociceptive action of adenosine itself in the facilitated state evoked by formalin and, vice versa. If fundamentally different mechanisms jointly contribute to the observed actions of two drugs on a given endpoint, such as antihyperalgesia, a synergistic interaction is considered likely. However, if mechanisms of action of one drug may be involved in those of another drug, a synergistic interaction may not be expected. It has been reported that adenosine may decrease excitatory amino acids release and inhibit the NMDA-mediated synaptic transmission or NMDA current (24-26), which suggest that the NMDA receptors may be affordable to the antinociceptive action of adenosine. As above mentioned, gabapentin may act on the NMDA receptors. Therefore, it could be assumed that the NMDA receptors may be linked to the antinocicpetive action of gabapentin and adenosine. Additionally, it has been reported that adenosine receptors were involved in the antinociception of gabapentin (4). These observations suggest that gabapentin and adenosine may have common pharmacologic sites of action. Thus, gabapentin may not interact with adenosine in a synergistic fashion. Another possible factor determining the properties of drug interactions may be the stimulus intensity of nociception. Previous report has shown that morphine interacts synergistically with pentobarbital at a low intensity stimulus, while interacting additively at higher intensity stimulus (27). The extent of antinociception produced was greater with the lower stimulus intensity (28). Hence, injection of lower concentrations of formalin, which are believed to be a milder stimulus, would reveal a synergy.
In conclusion, gabapentin and adenosine exhibit a parallel profile of spinal antinociception in the facilitated state without affecting motor function while interacting with each other in an additive manner.



 XML Download
XML Download