

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Metastatic breast cancer (MBC), one of the most common cancers affecting women, is regarded as largely incurable (1). Many chemotherapeutic agents have shown antitumor activity in MBC, among which the anthracyclines have been considered standard therapy (2, 3). Recently, taxanes have been reported to have efficacy in treating patients with MBC including individuals previously treated with anthracyclines (4). Few treatment options are available, however, for patients with MBC who have failed both anthracycline- and taxane-based chemotherapy regimens, or who face increased risk of developing anthracycline toxicity from further cumulative doses. Due to the poor overall outcome for patients with MBC, the aim of salvage chemotherapy is palliation of symptoms and improvement of quality of life. Thus, active agents with minimal toxicity are required for these patients.
Vinorelbine, a semisynthetic vinca alkaloid, has been considered one of the most active cytotoxic drugs against MBC, with a low toxicity profile. Vinorelbine has been found to yield response rates of 34-50% as a single agent when used as first-line therapy, and 15-30% as second-line therapy (5-11). The combination of vinorelbine and infused 5-fluorouracil (5-FU) has been acknowledged as an effective palliative regimen for MBC, especially in Europe, and has been tested in several phase II studies (12-15). Although this regimen showed high response rates, up to 70%, as first-line therapy, treatment tolerance was not satisfactory.
Capecitabine (Xeloda®), a fluoropyrimidine carbamate, was developed as an orally active agent that would deliver 5-FU selectively to the tumor tissues, and that would replace the more cumbersome infused 5-FU. In phase I/II studies, capecitabine gave response rates of 20-30% in patients with paclitaxel-refractory MBC, along with minimal bone marrow suppression (16-18). Capecitabine is also suitable for combination with a variety of agents, particularly those known to further upregulate thymidine phosphorylase (TP) in tumor tissue, such as paclitaxel, taxotere, and mitomycin-C (19-21). Several phase I/II studies using combinations of capecitabine and taxanes have demonstrated the high efficacy and safety of these regimens in MBC (22-24). Recently, data from a xenograft model indicated synergistic activity of capecitabine and vinorelbine by upregulation of TP in tumor tissue (25).
Due to their different mechanisms of anti-tumor activity, their differing toxicity profiles, and synergistic effect of both drugs, the combination of capecitabine and vinorelbine would be a reasonable choice for chemotherapy of MBC. There have been few reports, however, on this combination regimen although several phase I or II studies are ongoing (26-29).
We have had some experience with 3 week cycles of oral capecitabine (2,500 mg/m2/day on days 1-14) and intravenous vinorelbine (25 mg/m2/day on days 1 and 8) as last-line treatment in MBC. We found that this regimen was effective and well tolerated, although some patients could not receive the day 8 dose of vinorelbine due to myelosuppression. We therefore performed a prospective study to see the efficacy and safety of this combination chemotherapy in MBC patients previously treated with both anthracycline- and taxane-containing regimens. Preliminary results of this study were previously published in an abstract form (30).
MATERIALS AND METHODS
Patient Selection
Between April 2000 and September 2002, female patients with MBC were enrolled if they had measurable disease [i.e. a tumor having at least one diameter ≥2 cm by clinical examination, chest radiography or conventional computed tomography (CT) scan], or assessable disease, which was difficult to measure but could be evaluated grossly [i.e. by having diffuse small and numerous metastases in the liver or lung, or bone metastases]. All patients were ≥20 yr of age, had a performance status of 0-2 on ECOG scale, and had a life expectancy of at least 3 months. All patients were previously treated with anthracycline- and taxane-containing regimens, to which the disease was primarily refractory, or the patients relapsed after initial response. All patients had adequate hematologic function (absolute neutrophil count (ANC) ≥1,500/µL, platelet count ≥75,000/µL), hepatic function (total bilirubin ≤2.0 mg/dL, serum transaminase ≤3 times the upper normal limit (UNL) or ≤5 times UNL in cases with hepatic metastases), and renal function (serum creatinine ≤1.5 mg/dL). Patients who had received high dose chemotherapy and stem cell transplantation were eligible.
Exclusion criteria included patients who were pregnant or lactating, those with central nervous system metastases, patients with a prior history of other cancers within the previous 5 yr, aside from basal cell or squamous cell carcinoma of the skin, or carcinoma in situ of the uterine cervix, and those with significant gastrointestinal disease that could cause significant malabsorption or could affect drug intake. Patients could not have received chemotherapy, hormonal therapy or radiotherapy less than 4 weeks before study entry. The protocol was approved by the Institutional Review Board of Asan Medical Center. All patients gave written informed consents.
Treatment schedule
Each 3-week cycle of chemotherapy consisted of oral capecitabine (1,250 mg/m2 twice daily), according to the standard intermittent schedule (2 weeks of treatment followed by a 1-week rest period), plus intravenous vinorelbine, infused within 5-10 min at a dose of 25 mg/m2 on days 1 and 8 of each 3-week treatment cycle. Prophylactic colony stimulating factor was not permitted. Duration of treatment was based on response, and the study was initially designed so that patients with objective responses or stable disease would continue to receive chemotherapy unless the disease progressed or unacceptable toxicities occurred. Due to financial and insurance problems, however, patients who maintained a tumor response or stable disease beyond 6 cycles of chemotherapy were allowed an interruption and observation.
Palliative radiotherapy was not allowed until progression.
Toxicities and dose modification
Toxicity was graded before each treatment cycle according to the National Cancer Institute of Common Toxicity Criteria (31). The capecitabine dose was adjusted for non-hematological toxicities as outlined in Table 1. Dose adjustment criteria for vinorelbine was based on hematologic toxicities evaluated on days 1 and 8 of each cycle. If grade II neutropenia or thrombocytopenia had occurred on day 8, the vinorelbine dose delivered that day was reduced by 50%, whereas, if grade III/IV neutropenia or thrombocytopenia occurred, vinorelbine was not administered. If neutropenia greater than grade I had occurred on day 1, the treatment cycle was delayed for one week and then resumed at the same dose after resolution to grade I or better. If day 1 chemotherapy with either drug was delayed due to toxicity, administration of the other was also delayed, such that capecitabine and vinorelbine were started together on the same day of each cycle.
Pretreatment and follow-up evaluation
Prior to the first cycle of chemotherapy, each patient underwent a baseline assessment, including a complete medical history and physical examination, chest radiography, liver ultrasonography, and bone scan. CBC was performed on days 1 and 8 of each cycle, and blood chemistry tests were performed on day 1 of each cycle. Compliance for administration of capecitabine was monitored by questioning patients at each outpatient visit and counting their remaining pills at each cycle.
Response evaluation
In patients with measurable disease, response was assessed every 3 cycles using standard WHO criteria. The measurable disease by physical examination was assessed at each cycle. Complete response (CR) was defined as the disappearance of all known diseases, whereas partial response (PR) was defined as a 50% reduction of measurable disease. Progressive disease (PD) was defined as a 25% increase of measurable disease or the development of new lesions, and all other outcomes were assessed as stable disease (SD).
In patients with assessable disease, response was assessed when follow-up imaging studies showed obvious decrease in size and/or number of lesions, as judged by radiologists, and by improvement of symptoms. Response was categorized as improved, stable, or progressed.
Statistical analysis
The primary end point was response rate, and all eligible patients were included in the intention-to-treat (ITT) analysis of efficacy. This study was designed such that the expected response rate was 40% and so that the study would be halted if the response rate was 20% or less. According to Simon's two stage phase II design with α and β errors of 0.05 and 0.20, respectively, a minimum of 13 patients would be required to terminate the study as early as possible if the response rate was 20% or less for the first stage of the study (≤3/13). Otherwise, 43 patients would be required, and the study would be terminated if 12 or fewer responded to this regimen. Since we expected a non-compliance rate of 10%, we planned to enroll a total of 48 patients.
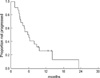
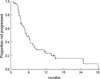
Progression-free survival (PFS), overall survival (OS) and duration of response were estimated as secondary end-points by the Kaplan-Meier method. The duration of response was measured from the date of documented response to the onset of PD; PFS times were determined from the date of entry to the study to the date of PD or death; and OS was measured from the date of entry to the date of last follow-up or death.
RESULTS
Patient characteristics
Between April 2000 and September 2002, 48 patients were enrolled into the study. Four of these patients were found to be ineligible: two had brain metastases, one did not have baseline data prior to the start of chemotherapy, and one patient showed very poor performance status (ECOG >2). The characteristics of the remaining 44 patients are shown in Table 2. The median age of all patients was 45 yr (range, 29-75 yr). Twenty-six patients had measurable disease, whereas 18 patients had only assessable disease. Combination therapy for metastatic disease was administered to 22 patients as second- line treatment, 19 as third-line treatment, and 3 as fourth-line treatment. A total of 235 cycles were administered (median, 5 cycles per patient; range, 1-24). All 44 patients were evaluable for toxicity and 43 patients for response, with 1 patient refusing evaluation of response after 3 cycles of chemotherapy.
Efficacy and survival
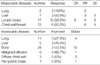
ITT analysis was applied to assess the response rate in all 44 patients (Table 3). Among the 26 patients with measurable disease, CR was observed in 1 (3.8%) with lung and neck lymph node metastases, and PR in 13 (50%), yielding an objective response rate of 53.8%. Among the 18 patients with assessable disease alone, 8 patients (44.4%) had improvement of symptoms with an obvious tumor response by imaging studies. Thus, the overall response rate in the ITT population of 44 patients was 50.0% (22/44, 95% CI, 35.0-65.0%). Response rates according to the metastatic sites are listed in Table 4.
Toxicity and dose intensity
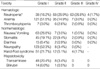
We found that, during the 235 cycles of chemotherapy, hematologic toxicity was the most common adverse reaction with grades III and IV neutropenia observed in 63 (26.8%) and 4 (1.7%) cycles, respectively, and in 30/44 (68.2%) patients. Only 1 patient, however, had febrile neutropenia, which was quickly reversible. There were no other admissions to the hospital for the treatment of infections or other toxicities. Grades II and III hand-foot syndrome occurred in 16 (6.8%) cycles, and in 10 (22.7%) of patients. Other nonhematologic toxicities were minimal and manageable (Table 5).
The dosage of capecitabine had to be reduced in 18 cycles of 11 patients due to grade II or III hand-foot syndrome (12 cycles) or grade II or III stomatitis (6 cycles). Dose reduction of vinorelbine on day 8 was required during 75 cycles (31.9%), 68 for grade II neutropenia, 4 for grade II/III stomatitis, and 3 for neurotoxicity. Vinorelbine on day 8 could not be given during 50 cycles (21.3%), 46 for grade III/IV neutropenia, 3 for poor vein status, and 1 for another reason. Chemotherapy had to be delayed in 82/235 (34.9%) cycles, primarily due to hematologic toxicity (65 cycles), but it was delayed for personal reasons in 15 cycles and for hand-foot syndrome in two. The median relative dose of capecitabine was 81.3% (range, 47-100%), whereas that of vinorelbine was 68.0% (range, 38-100%) of the planned doses.
DISCUSSION
With the widespread use of anthracyclines as adjuvant chemotherapy or first-line treatment of MBC and taxane-based regimens as salvage treatment, medical oncologists face difficulties in deciding how to treat MBC patients previously treated with these drugs. We have shown here that the combination of capecitabine and vinorelbine is highly active, achieving objective responses of 50% and a median response duration of 6 months in patients who had undergone both anthracycline- and taxane-based regimens. This response rate is very encouraging in this group of patients.
We found that although neutropenia was a frequent adverse event of this treatment regimen, it was relatively mild, with grade III occurring during 26.8% of cycles and grade IV during 1.7%, and, febrile neutropenia occurring only once in 1 patient. In addition, while hand-foot syndrome occurred in 24 (54.5%) patients and during 67 (28.5%) cycles, grade III toxicity occurred only during 4 cycles. Other non-hematologic toxicities were also minimal, and our patients went through treatment without serious complications, although dose modifications were necessary. Our findings indicate that this regimen was much less toxic than other regimens, including the combinations of adriamycin and cyclophosphamide, and adriamycin and taxane, as well as any combinations that include platinum.
Relative to the planned doses, the median relative dose of vinorelbine was 68.0% and that of capecitabine was 81.3%. The median dose intensity of capecitabine in our study did not differ much from the 77% observed during combination treatment with capecitabine and docetaxel (32). In that study, the combination of capecitabine and docetaxel achieved a response rate of 42% and a median time to progression of 6.1 months, as well as better survival than observed with docetaxel alone. And dose modification of capecitabine did not have a negative effect on response rate. A recent phase II study reported a response rate of 40% with the combination of capecitabine (2,000 mg/m2/day for 2 weeks) and vinorelbine (25 mg/m2 on days 1 and 8) in MBC patients previously treated with anthracycline and/or taxane (26). These data suggest that it may be possible to reduce the dose of capecitabine when it is combined with vinorelbine. In addition, our finding of a 50% response rate with a 68% relative dose intensity of vinorellbine, and, in many cases, the elimination of the day 8 doses, suggests that the dose of vinorelbine can also be reduced in heavily pretreated patients.
In our protocol, the dosage of vinorelbine was to be reduced by 50%, instead of 25%, on day 8 for grade II neutropenia, and no vinorelbine was to be given on day 8 in patients with grade III neutropenia. This is a somewhat aggressive dose modification. Although the proper dose schedule of this regimen was not clearly determined during the previous phase I studies, capecitabine 2,000 mg/m2/day for 2 weeks and vinorelbine 25 mg/m2/days 1 and 8 every 3 weeks has been generally recommended in this setting (27-29). A recent phase II study using this dose schedule showed, however, that treatment delay or dose reduction due to myelosuppression was common, resulting in reductions of dose intensity of capecitabine to 78% and vinorelbine to 82% of planned doses (26).
Our study included patients who had been previously treated with several chemotherapy regimens, suggesting that use of capecitabine and vinorelbine as first-line treatment for MBC may result in greater tolerability and less hematologic toxicity, as well as a better response rate than ours. Among the commonly used first-line regimens are adriamycin and paclitaxel (AT), fluorouracil, adriamycin and cytoxan (FAC), and adriamycin and cytoxan (AC), which have been reported to have response rates of 54-68% (33, 34). These regimens, however, have been associated with grade IV neutropenia in 27-89% of patients, and febrile neutropenia in 5-32% of patients, much higher rates than we observed here with capecitabine and vinorelbine. Since our regimen was very effective and had a low toxicity profile as a second or third line treatment, it would be of interest to determine whether a better response rate would be obtained if one moves our regimen up one step to be tried on patients previously treated with anthracycline but not taxane, and then compare this regimen to the combination of capecitabine and docetaxel. It would also be of interest to determine the efficacy of our regimen as a first-line treatment. The results shown here indicate that, even as a second or third line treatment, the combination of capecitabine and vinorelbine has merit for patients with MBC who cannot tolerate the severe toxicity of other treatment regimens.
In conclusion, we have shown here that, in treating MBC, the combination of capecitabine and vinorelbine is very effective and has low toxicity as a second or third line treatment.



 XML Download
XML Download