

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The metabolic syndrome, also called "syndrome X", "insulin resistance syndrome", or "cardiometabolic syndrome", refers to the state in which metabolic risk factors for cardiovascular diseases are clustered in individuals. The factors include abdominal obesity, atherogenic dyslipidemia, raised blood pressure (BP), insulin resistance, prothrombotic state, and proinflammatory state (1).
Since the work of Reaven (2), the evidences that the metabolic syndrome increases the risk for morbidity and mortality of cardiovascular disease have accumulated (3-5). Studies have shown that metabolic factors tend to aggregate in individuals, and that clustering is more harmful than having an individual single factor.
Unfortunately, prevalence of insulin resistance or type 2 diabetes has increased on a worldwide level, especially in non-Europe, Asian regions. This phenomenon has been called "diabetes epidemic" (6). However, nationwide prevalence of the syndrome or its relationship with cardiovascular diseases has not yet been reported in Korea. Previous studies involved subjects who were either the residents of specific localities (7, 8) or voluntary clients of a university hospital (9-13), and therefore the estimates could not be generalized. Moreover, different case definitions used in these studies set limits to comparison.
This study was undertaken to estimate the nationwide prevalence of the metabolic syndrome and its individual components among Korean adults, and to explore its relationship with cardiovascular diseases.
MATERIALS AND METHODS
Data collection
In 1998, the first Korea National Health and Nutrition Survey was conducted. It involved a health interview survey, health behavior survey, and dietary survey by home visits and health examination survey at local centers. Anthropometric measurement including height, weight, waist circumference (WC), and hip girth was performed. Systolic and diastolic BP were measured twice using a sphygmomanometer at phase I and V, respectively, and were averaged. The subjects went through more than 10 hr fasting and blood samples were obtained using venupucture. The blood samples were analyzed for serum total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL), and fasting blood glucose (FBS) (Hitachi-747 autoanalyzer; Hitachi, Japan). In addition, current medication status for hypertension or diabetes, personal history of cardiovascular disease including cerebrovascular disease and ischemic heart disease, and family history of diabetes, cerebrovascular disease, or ischemic heart disease were determined by self-reports.
The subjects were selected based on stratified multistage probability sampling, and generalization to the general population of Korea is possible. We analyzed the data of 2,731 men and 3,416 women aged 25 yr and over who completed all the items of health examination. In order to estimate nationwide prevalence we applied sample weights proposed by Korea Institute of Health and Social Affairs (14).
Case definition
The metabolic syndrome was defined according to 2001 National Cholesterol Education Program Adult Treatment Panel III (ATP III) (1), except for abdominal obesity by WC which did not seem applicable to relatively lean Asian people. WC is known to directly reflect abdominal fat mass and to have a good correlation with other metabolic components (15), and Inoue et al. proposed WC standard for Asians (16). However, Bjorntorp reported that actual cardiovascular risk is more correlated with waist-to-hip ratio (WHR) than WC because the former includes hip girth reflecting muscle mass important in insulin regulation as well as WC reflecting abdominal fat (17). The World Health Organization (WHO) proposed the WHR standard to determine the metabolic syndrome in 1998 (18). Hence, in this study, we used both WHR and WC to fix two kinds of definitions for the metabolic syndrome, and compared the results (19). The syndrome was defined as having 3 or more components from the following: 1) abdominal obesity (a) WC ≥90 cm in men and 80 cm in women (16), or (b) WHR >0.9 in men, and 0.85 in women (18); 2) high TG ≥150 mg/dL; 3) low HDL <40 mg/dL in men, and <50 mg/dL in women; 4) high BP ≥130/85 mmHg or current medication; and 5) high FBS ≥110 mg/dL or current medication (1).
Other metabolic abnormalities were defined as: 1) high TC ≥240 mg/dL; and 2) high low-density lipoprotein cholesterol (LDL) ≥160 mg/dL (1).
Cardiovascular cases were determined based on self-reports, in which the participants stated that they were affected by cerebrovascular diseases, ischemic heart disease, or other heart diseases.
Statistical analysis
The prevalence of the metabolic syndrome and its individual components was calculated using sample weights to obtain the nationwide representative estimates.
Theoretically, prospective studies are necessary in order to identify the causal association between the syndrome and cardiovascular diseases, but this could not be done in this study. Therefore, the cross-sectional associations between them were examined (19). Age-adjusted odds ratios (ORs) of metabolic abnormalities for cardiovascular disease and covariates-adjusted ORs were estimated using logistic regression models. The covariates were chosen through stepwise selection among age, family history of hypertension, diabetes, or ischemic heart disease (yes or no), depression (never, often, or always), smoking (never, ex, or current smoker), drinking (never, ex, or current drinker), weight change (constant, increase, or decrease), regular exercise (vigorous, moderate, or never), lifestyle (active, modest, or sedentary), and carbohydrate intakes (<60, 60-70, or >70% of total energy intake). All analyses were performed separately according to gender using SAS version 8.1.
RESULTS
Table 1 shows the anthropometric and metabolic characteristics of the participants. The average levels of WC, WHR, systolic and diastolic BP, and TG were much higher in men than in women, and those of hip girth, body mass index (BMI), and TC did not significantly differ between gender. However, HDL and LDL levels were higher in women. Because these samples were representative, the estimates indicated the current level of national averages, and even after age-standardization, the gender differences remained alike except for LDL and FBS. Though crude comparison with American whites (obtained from NHANES III, 1988-1994) (15) without considering demographic structure is questionable, the BMI of Korean men and women was lower than that of American whites on the average: 23.2 vs. 26.6 kg/m2 in men, and 23.4 vs. 26.3 kg/m2 in women. As for abdominal obesity, WC of Korean men and women (83.2 and 78.8 cm) was smaller by 12-16 cm than that of American men and women (97.9 and 89.6 cm, respectively). In addition, Americans showed more adverse lipid profiles, such as higher TC, TG, and LDL. However, BP level was higher in Koreans, and FBS level did not seem to differ much between them (Table 1).
Table 2 shows the distribution of overlapping abnormalities. The proportion of subjects having at least one component was over 75%. As the number of abnormalities increased, prevalence decreased. Among men, prevalence of abdominal obesity by WHR standard was higher than that by WC, but there was no difference in women. Prevalence of the metabolic syndrome, defined as having 3 or more components, was 22.1% (by WC) and 28.6% (by WHR) in men, and 27.8% (by WC as well as WHR) in women (Table 2).
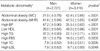
Table 3 presents the prevalence of the metabolic abnormalities. Prevalence of abdominal obesity based on WC and WHR differed considerably in men but not in women. If the WC standard was used, prevalence of women was nearly twice that of men, but if WHR was used the prevalence did not differ much (p=0.460). Those of low HDL (49.0%), high TC (9.8%), and high LDL (9.7%) were higher in women, while high BP (47.2%), high TG (37.3%), and high FBS (22.1%) were more prevalent in men (all p<.01). Even after age-standardization, the pattern remained alike (Table 3). Among the cases of metabolic syndrome, high TG and high BP were remarkably prevalent (over 75%) in men, while low HDL, abdominal obesity, and high BP were in women (data not shown).
To explore prevalence differentials caused by abdominal obesity standards, the relationship among WC, hip girth, and WHR were examined according to age group and gender. As shown in Fig. 1, in men, both WC and hip girth decreased slowly with age, but the slope in hip girth was more steeper, resulting in the rise of WHR with age. On the contrary, in women, while hip girth seemed constant across age groups, WC rise was remarkable, also giving WHR increase with age (Fig. 1).
Fig. 2 shows the age-specific prevalence of the metabolic syndrome and its individual abnormalities. Prevalence of abdominal obesity by WHR, high BP, high TG, and high FBS was higher in men than in women among the age groups under 55 yr. However, its rise according to age was steeper in women. Therefore, among the groups over 55 yr, prevalence was much higher in women. Low HDL and abdominal obesity based on WC was more prevalent in women across all age groups. Age-specific prevalence of the metabolic syndrome in men increased to 54 yr old, followed by decrease or plateau. On the contrary, women had lower prevalence in the beginning, but the increase according to age continued on after 55 yr old (Fig. 2).
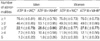
The relationship between the metabolic abnormalities and cardiovascular diseases is shown in Table 4. Covariates-adjusted ORs of the syndrome were 1.97 (95% CI 1.26-3.09, by WC) and 1.48 (0.96-2.28, by WHR) in men, and 1.54 (1.15-2.07, by WC) and 1.31 (0.97-1.75, by WHR) in women. The impact of adjustment for covariates was not large. The covariates-adjusted ORs of the syndrome by WC was larger than that by WHR in both genders, and also larger than those of individual abnormalities (Table 4).
DISCUSSION
This study analyzed a national representative sample obtained from the first nationwide health examination survey in Korea 1998. External validity is therefore sufficient to interpret the findings for the general population of Korea.
As shown in Table 1, attributes of body physique and metabolic factors were very different from American whites, therefore the case definition based on ATP III had to be modified. Since there was no universal agreement, two different standards were used for abdominal obesity (16, 18, 19), by which the prevalence difference was large in men but was almost negligible in women (Table 2, 3). This phenomenon seemed to result from the relationship among WC, hip girth, and WHR. In women, WHR increase was pulled by WC rise, while in men it was caused by disproportional decreases of hip girth to WC (Fig. 1).
According to Table 2 and 3, metabolic abnormalities are very prevalent among Koreans, and roughly up to 8 million adults are supposed to be affected by the metabolic syndrome. The estimated prevalence of this study was higher than previously reported in Korea, being 9.8-20.8% in men and 10.3-19.6% in women (7-13). Such difference partly resulted from different case definition; for instance, two studies (7, 8) were conducted before ATP III recommendation, and one study (9) used ATP III with BMI standard instead of abdominal obesity. However, more important reason of different results lies in selection bias; although three studies (10, 11, 13) used the same criteria as we applied, which means ATP III with abdominal obesity standard for Asians, the estimated prevalences were much lower than ours. The subjects of those studies were recruited among the clients of comprehensive medical examination in a university hospital, which implied that they were likely to be younger and healthier, or having higher social status so they could not represent general population in Korea. In that socioeconomic factors are related to the metabolic syndrome (20), the previously reported prevalences seem to be underestimated.
In addition, estimate in the present study was higher than that of American whites, which was 24.8% in men and 22.8% in women (21). Such difference partly resulted from the difference in the case definition used (i.e., abdominal obesity) or demographic structure. However, some studies showed that Asians are more vulnerable to the metabolic risk compared to Caucasians. Various studies comparing Asian ethnics, such as Filipinos (22), Japanese (23, 24), and South Asians (25) with Caucasians reported that Asians had higher risk of diabetes or metabolic syndrome although they were less obese. This study also supports such findings.
Even though the prevalence of the syndrome in men and women was approximate, age-specific prevalence of the syndrome and its individual abnormalities significantly differed (Fig. 2). In men, a plateau or decrease was observed in the age groups over 55 yr, which was supposed to reflect cohort effect or selective survival. On the contrary, in women, prevalence continuously increased with age, which could in part be an effect of menopause. Although menopausal status was not included in the survey, there was another study that reported visceral fat accumulation and acute increase of insulin resistance after menopause (23).
For the association with cardiovascular diseases, the metabolic syndrome was found to be positively related. The effect size of the metabolic syndrome by WC standard was larger than that by WHR, and the former seemed to have more closer relationship. When using WC standard, the covariates-adjusted OR of the syndrome in both gender was larger than individual abnormalities, which agreed with the previous findings that clustering of metabolic factors is more harmful than having an individual single factor (3-5). However, because the analysis was cross-sectional and the case definition of cardiovascular diseases was based on self-reports, no clear decision could be made.
Whatever, in relation to population impact determined by prevalence and effect size, control and prevention of the metabolic syndrome is important for prevention of cardiovascular disease in Korea. Although higher risk of women observed in other studies (3, 4) was not identified in this study, it is still important to focus on women because prevalence of the syndrome was considerably high in elderly women.
In conclusion, this study shows that, no matter what standard for abdominal obesity was used, representative prevalence of the metabolic syndrome among Korean adults was higher than previous reported, and moreover, also higher than that of American whites who are more obese than Koreans. According to the results, current cases might be up to 8 millions in Korea, and they are supposed to have more risk for cardiovascular diseases. We would like to recommend that usual health examination include assessment of the metabolic syndrome, and based on that, secondary prevention be implemented immediately, especially among elderly women. Further studies are necessary to define the level of metabolic abnormalities to predict cardiovascular risk among relatively lean Asians and to unravel determinants of the syndrome for primary prevention.




 XML Download
XML Download