

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Hypothermia defined as a core body temperature <35℃ can be a life-threatening emergency, especially in cold winter climates, but can be used therapeutically. Therapeutic hypothermia (TH) has been used to improve neurological outcome in comatose patients after cardiac arrest.1)2) The exact mechanism for neuroprotection is unclear; potential mechanisms include attenuation of deleterious processes occurring after initial hypoxic tissue injury.3)4)5)
Generally, mild hypothermia is defined as a core body temperature between 32℃ and 34℃.2) This is thought to be appropriate temperature between neuroprotective effects and possible toxicities. The Osborn wave (also known as the J wave) is an established electrocardiogram (ECG) manifestation of hypothermia. It is not pathognomonic of hypothermia, but usually occurs in patients with a core temperature <32℃ and the magnitude of the J point elevation correlates inversely with the body temperature.6)
Several studies have suggested an arrhythmogenic potential of the Osborn wave,7)8)9)10) but there is no solid evidence that TH-induced Osborn wave itself is associated with increased mortality.11)12) Here we report a case of recurrent ventricular fibrillation (VF) after appearance of Osborn wave during mild TH.
Case
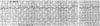
A 56-year-old man with no underlying disease was admitted to the emergency department with sudden cardiac arrest. While having breakfast, he suddenly pounded his chest. His wife noticed he was cyanotic and having difficulty breathing. He received cardiopulmonary resuscitation (CPR) from his son for about 20 minutes until paramedics arrived with a defibrillator. The initial rhythm was VF (Fig. 1). Defibrillation with 200 J was delivered once followed by 5 cycles of CPR. Following restoration of cardiac rhythm, he was transferred to a hospital where he was intubated. The initial ECG finding was sinus tachycardia. He was transferred to our hospital for further management.
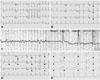
At our hospital, initial ECG (Fig. 2A) showed sinus tachycardia with a heart rate of 114 beats per minute. On the first day of admission, echocardiography was done, which showed no regional wall motion abnormality of the left ventricle. The ejection fraction of left ventricle was 60%. Chest and brain computed tomography (CT) also did not reveal abnormality. The initial pH was 7.375 and the levels of electrolytes including sodium, potassium, calcium and magnesium were within the normal ranges.
Therapeutic hypothermia was conducted after transfer to the intensive care unit. The target temperature was 33℃. Soon after TH was begun, Osborn waves appeared in lead II and V 4, V 5, and V 6 (Fig. 2B). Two hours after TH, VF occurred when the esophageal temperature was 34.9℃. Defibrillation of 150 J was applied (Fig. 2C). Not much later atrial fibrillation developed and the Osborn waves were prominent in diffuse leads. Three more defibrillations were delivered to terminate VF and the height of Osborn waves increased over time (Fig. 2D and E). TH was halted due to recurrent VF. Two hours after a warmer was applied to the patient, ECG revealed less prominent Osborn wave and VF did not recur.
Two days after admission, the patient was extubated. He was alert and had no neurological deficit. Several days after, a coronary angiography revealed no significant narrowing in coronary vessels. An ergonovine provocation test was also done to see if coronary vasospasm had occurred. The result was negative. There was no induced ventricular tachycardia (VT) at electrophysiological study. The ECG several days after admission didn't show abnormality (Fig. 3A). He was diagnosed with idiopathic VF and discharged from our hospital after implantable cardioverter defibrillator insertion (Fig. 3B).
Discussion
It is generally accepted that TH has the potential to improve the neurological outcome in comatose patients after cardiac arrest.1)2) Following initial resuscitation, various mechanisms including ischemia, reperfusion injury, inflammatory response, and free radical production are involved in cerebral damage.1)3)5) TH lowers the cerebral metabolic rate, blocks the apoptotic pathways, suppresses inflammatory responses, and attenuates production of free radicals.3)4)5) However, possible side effects, such as electrolyte imbalance, hemodynamic instability, infection, seizures, and arrhythmias, can rarely occur in patients undergoing TH.1)2)5)
Electrocardiogram findings of hypothermia include Osborn waves, atrial and ventricular dysrhythmias, and interval (PR, QRS, QT) prolongations.11)13)14) Among these, the Osborn wave is a positive deflection occurring at the QRS-ST junction and may originate from a transmural voltage gradient during early repolarization due to a transient outward potassium current in the epicardium, but not in the endocardium.15) As the Osborn wave can be seen in various conditions like acidosis, subarachnoid hemorrhage, and hypercalcemia, it is not pathognomonic of hypothermia. But, it has been reported that the height of J point elevation is related with the severity of hypothermia.6)
Several mechanisms have been suggested to explain the arrythmogenic potential of the Osborn wave. The prominent action potential notch can lead to loss of the dome of action potential, which can heterogeneously cause a marked dispersion of repolarization. This eventually can cause extrasystolic activity by a mechanism called phase 2 reentry and VF.15)16) Another proposed mechanism is triggered automaticity. Intracellular Ca2+ overload during hypothermia is a precursor for early or delayed after depolarization, which is associated with triggered activity.17) However, other reports have not associated the Osborn wave with VF in hypothermic patients.18) Therefore, the arrythmogenic potential of the Osborn wave requires further study.
Although various adverse events have been reported during TH, TH-induced arrhythmia seems not to be related with increased mortality.1)2) In one study of ECG changes in TH, the Osborn wave incidence during TH was 30% and no association with unfavorable short-term outcome was evident.11) After rewarming, the Osborn wave disappears in almost cases. So, on the basis of many studies, TH is well tolerated and relatively safe. Current guidelines recommend mild TH in comatose patients after cardiac arrest.
Hypothermia is also proarrhythmic and can cause lethal arrhythmias, especially at low temperature and in the presence of low serum pH.19) However, in our case, VF developed in normal serum pH, electrolyte levels, and not markedly low body temperature. Therefore, VF and Osborn wave seem not always to be related to body temperature, and individual variations in response to hypothermia can be more important to determine the vulnerability to arrhythmias. Physicians need to monitor patient's vital signs including core temperature, ECG, and laboratory tests carefully during TH.

 XML Download
XML Download