

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Juxtaglomerular cell tumor (JCT) of the kidney, also called reninoma, is a rare benign renal neoplasm, which itself is a rare cause of secondary hypertension.1) The neoplasm is usually found in young adults in their 20s or 30s. Reninoma produces inordinate amounts of renin and consequently induces secondary hyperaldosteronism, hypokalemia, and hypertension. Because reninoma is a curable cause of hypertension by surgical resection, accurate diagnosis and treatment is highly important. We describe a case of secondary hypertension with a single renal mass in a 21-year old man.
Case
A 21-year-old man was referred to our hospital due to progressively worsening headache of two-month duration. He was diagnosed with hypertension 7 years ago and was treated with angiotensin II receptor blocker (ARB) and calcium channel blocker. His mother had a history of hypertension. The headache had become gradually aggravated during the prior 2 months, and was associated with dizziness. He did not complain of any coughing, hemoptysis, abdominal discomfort, nocturia, sweating, or focal neurological symptoms.
On admission, blood pressure and heart rate was 152/108 mmHg and 76 beats/min, respectively. His height was 175 cm and weight was 91 kg. Physical examination revealed normal lung and cardiac sounds. Abdominal bruits, tenderness, or masses were not observed.
Initial laboratory findings revealed normal blood urea nitrogen (17 mg/dL), serum creatinine (1.1 mg/dL), sodium (137 mmol/L), potassium (3.5 mmol/L), fasting glucose (175 mg/dL), and calcium (8.8 mg/dL). Electrocardiogram and chest x-ray showed normal sinus rhythm and unremarkable radiographic findings. Echocardiographic features were normal, without evidence of heart failure or aortic coarctation. Twenty four hour urinary catecholamine and vanillymandelic acid level (5.3 mg) was within normal range. Plasma renin and aldosterone level were 6.67 ng/mL/hr and 11.09 ng/dL in the supine position, respectively and 9.96 ng/mL/hr and 20.47 ng/dL, respectively, when upright.
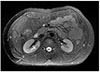
Kidney ultrasonography revealed no evidence of definite renal artery stenosis and computed tomography (CT) showed a well-defined mass, 1.7×1 cm in size, in the middle pole of the right kidney (Fig. 1). Magnetic resonance imaging (MRI) also revealed a 1.8 cm small and solid mass in the same right kidney (Fig. 2), which had iso-signal intensity in the T1-weighted image and heterogenous, mild, low signal intensity in the T2-weighted image. Whole body bone scan showed no active bone lesions.
The patient underwent partial nephrectomy to remove the mass in the right kidney. Grossly, the renal parenchyme was a well-demarcated and oval mass with gray fish flesh-like cut surface and focally hemorrhage, measuring 1.5x1 cm (Fig. 3). The lesion was close to the surgical resection margin and low mitotic figures were identified. On microscopic examination, a relatively well-circumscribed tumor was identified. Thick-walled blood vessels were well developed, with a characteristic hemangio-pericytic pattern. Immunohistochemically, vimentin and CD34 staining were positive. On electron microscopy, the tumor cells displayed numerous secretory granules, some of which showed typical rhomboid crystalline-material that was thought to be renin protogranules (Fig. 4). Consequently, this mass was confirmed as a juxtaglomerular cell tumor.
On the second day after surgery, the level of plasma renin decreased to 0.01 ng/mL/h and blood pressure had normalized (120/80 mmHg). The antihypertensive regimen was decreased (amlodipine 5 mg only) on discharge. At the 2-month follow-up, blood pressure (112/80 mmHg) and serum potassium level (4.3 mmol/L) remained normal.
Discussion
Reninoma is a rare cause of secondary hypertension. Since it was first described in 1967,2) about 100 patients have been reported.3) An epidemiologic study revealed that reninoma is mainly diagnosed in young adults (mean age 27 years) and more commonly occurs in female patients.4) The most common presenting symptom is headache, followed by dizziness, nausea, polyuria, and nocturia.
Typical reninoma patients show a clinical triad of hypertension, hypokalemia, and high level of plasma renin activity.5) Most of the patients present with hypertension at the initial examination, because of the high plasma renin level induced by the renal tumor. Hypertensive end-organ damage, such as retinopathy, papilledema, proteinuria, renal failure, and left ventricular hypertrophy, has also been commonly observed.4) Our patient was obese and had a family history of hypertension. Nevertheless, headache and early onset of hypertension raised suspicion for secondary causes of hypertension.
Dong et al.6) classified JCT into typical, atypical, and non-functioning types depending on blood pressure and serum potassium levels. The typical type was defined as a JCT with hypertension and hypokalemia. Atypical type was defined as hypertension without hypokalemia. Non-functioning type was defined as JCT without hypertension and hypokalemia. Laboratory findings of typical reninoma are high plasma renin activity, high aldosterone level, and hypokalemia. Repeated examinations of plasma renin and aldosterone levels according to postural changes are helpful in the diagnosis of a reninoma, but these results can be negative in atypical and non-functioning types.7) Our patient showed mild to moderate hypertension and mildly elevated plasma renin activity, but had normal serum aldosterone and potassium levels. According to this classification, our patient had an atypical type of reninoma. However, normal potassium levels in our patient could have been masked by ARB medication. Thus, it is difficult to conclude that the patient had a truly atypical type of reninoma.
Imaging tools are used to diagnose and localize the renal mass. Kidney ultrasonography and Doppler study is the first choice in the search for a renal mass or artery stenosis. Selective arteriogram can reveal a reninoma as a small avascular area in the kidney, but the sensitivity is low. CT scan is the most powerful imaging tool for this renal tumor, with 100% sensitivity.4) In this case, CT scan identified the lesion as an iso-dense small mass compared with the renal medulla, with mild and persistent enhancement in dynamic study. MRI is also highly effective in differential diagnosis between reninoma and other renal tumors.
Reninoma is usually confirmed by either positive immune-staining of renin or electron microscopic identification of renin granules.8) Specific immunohistochemical appearance of reninoma is positive staining for renin, actin, vimentin, and CD34.9) These histologic findings are typical and help to diagnose differentially between JCT and other renal tumors. The most specific electron microscopic findings are rhomboid crystalline protogranules or amorphous homogeneous, electron-dense mature granules.
Reninoma is usually benign, but increases the risk of cardiovascular complications. Thus, surgical resection of the tumor is initially considered. Nephron-sparing operation, such as partial nephrectomy, with tumor resection or radical nephrectomy is recommended.10) Laparoscopic partial nephrectomy is also considered because of less postoperative pain, less blood loss, and shorter hospitalization. Our patient underwent partial nephrectomy. We did not measure renin activity in the renal vein because renal vein sampling often fails to provide adequate localization of reninoma.11) Failure in localization may occur when a tumor is located at the surface of the kidney. Postoperatively, associated symptoms with reninoma are usually improved, and 90% of patients no longer requiring antihypertensive management.
The differential diagnosis of reninoma requires various diagnostic tools. Elevated plasma renin activity is not specific for reninoma. Several tumors, such as Wilms' tumor, clear-cell type of renal cell carcinoma, and lung cancer can produce extraphysiologic levels of renin. Also, atypical or non-functioning types of reninoma are associated with normal levels of potassium and aldosterone. Thus, additional imaging and pathologic confirmations are required to diagnose a reninoma. In this case, because the patient showed mildly elevated renin level with normal potassium and aldosterone levels, we suspected an atypical type of reninoma, which was confirmed on imaging and surgical resection.
Reninoma is a rare cause of secondary hypertension in young adults. Although the clinical triad of reninoma is hypertension, hypokalemia, and high level of plasma renin activity, atypical type of reninoma presents mild hypertension and normal potassium level, as in the present case. Thus, it is important to suspect reninoma even when potassium levels are normal and additional imaging study and surgical confirmation are necessary.



 XML Download
XML Download