

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Radiation exposure is an important health concern in the field of interventional cardiology. Modern cardiac catheterization equipment has several selectable variables that decrease the radiation doses delivered to patients during a cardiac procedure. A "Store fluoro" function is one of those variables (e.g. Siemens cardiac angiography system) that allows for the retrospective storage and replay of fluoroscopy images. Because the radiation doses delivered to patients are approximately 10-20 times lower in the fluoroscopy mode than in the conventional cineangiography mode, the dose can be minimized by the appropriate utilization of stored fluoroscopy images. This method is known as fluorography.1)
Coronary angiography (CAG) is the gold standard for diagnosing coronary artery obstructive disease (CAOD). Currently, cineangiography, which refers to CAG using cinematography for image acquisition, is the standard method and a major contributor to the total radiation dose delivered during CAG.2) However, current technology allows for improved visualization using fluoroscopy alone, through, for example, a "Store fluoro" function for saving fluoroscopy images for retrospective review. Hence, we hypothesized that the "Store fluoro" function effectively minimizes the total radiation dose of CAG, as compared with conventional cineangiography, and thus conducted this study to determine whether fluorography is truly effective in decreasing the radiation exposure during diagnostic CAG.3)
Subjects and Methods
Patients were enrolled who underwent elective CAG from July 1 to September 5, 2014, at the cardiac catheterization laboratory of the Pusan National University Yangsan Hospital. The excluded patients were those with a heart rate of >100 bpm and body mass index (BMI) of >30 kg/m2, because higher radiation doses are required to produce adequate image quality in such patients.4)5) Patients with a glomerular filtration rate (GFR) of <60 mL/min/kg were also excluded, in order to avoid an inadvertent overuse of the contrast agent. The remaining patients were prospectively enrolled into a cineangiography group or a fluorography group, in accordance with the professional opinion of a medical scientist. The procedures were performed by four operators who had performed CAG for >100 cases of percutaneous coronary intervention (PCI) during the past 1 year. In the fluorography group, if the image quality was not adequate to facilitate decision-making, hence images were acquired again using cinematography. This additional radiation exposure was included in the total radiation exposure for the fluorography group patients.
Routine CAG views were obtained by the operators as follows: anteroposterior (AP) caudal view, AP cranial view, left anterior oblique (LAO) cranial view, and LAO caudal view for the left coronary artery and LAO and AP cranial views for the right coronary artery. The Artis zee CAG system was used during all procedures; it was equipped with software version VC21B, lead shields (Siemens AG; Erlangen, Germany), and a ceiling-mounted lead shield.
The patients' baseline clinical characteristics and laboratory data were collected and the angiographic and procedural characteristics were recorded. The degree of coronary artery stenosis was visually estimated. The primary outcomes included radiation measurements in the form of air kerma (AK; mGy) at the interventional reference point (Ka, r) and the dose (AK)-area product (DAP; µGy · m2). The AK is defined as the kinetic (e.g., radiation) energy adsorbed per unit mass of air (kg), while the DAP is the product of AK and the exposed area.
The secondary outcomes included the total procedure time (time between vascular sheath insertion and removal) and the total amount of contrast agent used during a CAG.
For objective analysis of the angiographic image quality, three experienced interventional cardiologists (with a minimum of 4 years experience after completion of interventional cardiology fellowship training) reviewed the angiographic images. These cardiologists were blinded to the patient data and patient groups. The image quality was judged by an operator on a 10-point scale, where a score of 10 represented the ideal image quality for decision-making and a score of 1 represented an image quality that is not suitable for analysis. The recorded score represented a patient's entire study; individual images were not separately graded. Each participating interventional cardiologist reviewed five additional cases, common to all reviewers, and all the reviewers' quality scores were recalibrated from the median scores for the commonly reviewed cases. This was done to adjust for any interobserver variation.
Categorical variables are expressed as percentages and continuous variables as a mean±standard deviation. Differences in categorical variables between the two groups were analyzed using the χ2 test or Fisher's exact test, while the independent two-sample t-test was used for continuous variables. A two-sided p of 0.05 was considered statistically significant. All statistical analyses were performed using an SPSS version 18.0 (SPSS Inc., Chicago, IL, USA).
Results
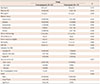
A total of 172 patients were enrolled, 90 of whom were excluded because they required additional procedures. From the remaining 82 patients, the following were also excluded: 10 with a heart rate of >100 bpm, 10 with a GFR of <60 mL/kg/min, and seven with a BMI of >30 kg/m2. Thus, in total, 55 patients, including 19 in the fluorography group and 36 in the conventional cineangiography group, were analyzed (Fig. 1). The baseline characteristics showed no significant differences between the two groups, except for a relatively higher heart rate and a higher incidence of CAOD in the cineangiography group, as compared with those in the fluorography group (Table 1). Almost all patients, except three, underwent CAG using the right radial artery.
The total AK and DAP were significantly lower in the fluorography group (159.3±64.9 mGy and 1337.9±629.6 µGy · m2, respectively) than in the cineangiography group (326.9±107.5 mGy and 2341.1±849.9 µGy · m2, respectively, p<0.001 for both; Fig. 2). The total procedure time (cineangiography vs. fluorography, 12.8±4.7 vs. 12.5±2.9 min, p=0.779) and amount of contrast agent used during CAG (136.1±28.3 vs. 126.3±25, p=0.214) were not different between the two groups (Table 2). The image quality for most patients in the fluorography group was adequate for decision-making (Fig. 3); only two (10%) patients underwent additional cineangiography as per the operator's discretion. However, this had no significant effect on the total radiation exposure.
The results of the analysis of angiographic image quality are presented in Table 3. There were no significant differences between the two groups in the unadjusted angiographic image quality scores (cineangiography group, 8.56±0.153; fluorography group, 8.36±0.435; p=0.063). When the angiographic quality scores were adjusted for potential interobserver variability in the image quality assessment, the fluorography group still showed a slightly lower quality score, although the difference was not statistically significant (cineangiography group, 8.43±0.152; fluorography group, 8.32±0.146; p=0.078). These results indicate that although the image quality in the fluorography group was lower than that in the cineangiography group, it was within acceptable limits.
Discussion
In this study, we demonstrated that fluorography was effective in decreasing the radiation exposure during CAG for selected patients. The total AK and DAP were significantly lower in the fluorography group than in the cineangiography group, although the total procedure time, and amount of contrast agent used, were not different. In addition, it showed an acceptable image quality that facilitated decision-making.
Ionizing radiation during CAG has serious negative biological effects on humans. These include deterministic effects, such as skin injury, and stochastic effects such as malignancy and congenital abnormalities.3) Radiation exposure has always been a serious health issue since the introduction of diagnostic cardiac catheterization and interventional treatment using radiation in the field of cardiology, although the associated biological hazards have been ignored for several reasons. First, the fact that ionizing radiation is invisible and does not cause any sensation during exposure. Second, there was a then prevalent altruistic philosophy that physicians should devote and sacrifice their lives for a patient's treatment. However, a high incidence of left-sided brain and head and neck tumors has recently been reported for physicians who perform daily interventional procedures in the presence of radiation, thus bringing these ignored issues back to the forefront of interventional cardiology.6)
Recently, some studies showed the effectiveness of fluorography in decreasing the radiation exposure during CAG. Shah et al.7) reported its association with a significantly decreased radiation dose (approximately 60% decrease in DAP), compared with that during cineangiography; while Olcay et al.8) showed that senior operators, experienced in intravenous ultrasound and fractional flow reserve, can safely use fluorography, even for coronary artery stenting, and that fluorography delivered a much lower radiation dose, used less contrast agent, and took less time compared with conventional cineangiography. Although fluorography has a number of disadvantages, the results of studies consistently showed a clinical effectiveness comparable with that of cineangiography. However, practices remain unchanged. To change the current clinical practice for the better, more evidence is required. It is averred that the results of this study have added robust evidence regarding fluorography. However, needless to say, radiation safety issues in the field of interventional cardiology should not be overlooked.
Some unique aspects of this trial include the fact that CAG was performed through the right radial artery in most patients, and the frequency of additional cineangiography in the fluorography group was relatively low. Furthermore, to the best of our knowledge, this is first trial in Asian patients who exhibited a BMI lower than that of patients in the other studies.
This study also has some limitations. Because it is not a randomized study, the results inevitably contain significant operator-dependent bias. Also, a relatively small number of clinically stable patients were enrolled. Thus, it remains unclear whether CAG using fluorography alone can be applied for all patients.
In conclusion, this study was initiated to discover reasonable ways of minimizing ionizing radiation during the treatment of patients; hence, a simple and effective method was identified that can protect the interventional cardiologist in daily clinical practice. To achieve this, we compared CAG using fluorography with CAG using conventional cinematography in terms of the radiation exposure. These findings showed a substantial decrease in the radiation dose and an acceptable image quality in the fluorography group. Therefore, we strongly recommend fluorography, based on a "Store fluoro" function of a CAG system, as a useful method for minimizing the radiation exposure in selected patients.





 XML Download
XML Download