

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Hypertrophic cardiomyopathy (HCM) has had a variety of names because of its diverse clinical manifestations since it was first described in detail by Braunwald et al. in 1964.1)2) Owing to these variations in the clinical course, the prognosis and natural course of HCM differs across patient cohorts. Few definite risk factors have been identified for morbidity and mortality in HCM, except a family history of sudden cardiac death (SCD). Recent studies have reported that the natural course of HCM, particularly in older age groups, is better than previously considered, irrespective of the presence of well-known risk factors.2)3)
Apical hypertrophic cardiomyopathy (AHCM) is an uncommon morphologic variant of HCM wherein the hypertrophy of the myocardium predominantly involves the apex of the left ventricle (LV).4)5) This entity is very rare in non-Asian populations, with most reports suggesting an overall prevalence of 1-3% in HCM patients.6)7)8)
Most AHCM patients present with mild or no symptoms and good prognosis.5)9) However, clinical presentations with wide QRS tachycardia, subendocardial myocardial infarction, atrial flutter, and LV aneurysm have been reported in some cases.10)11)12)13)14) Despite these reports, the natural course of AHCM remains obscure as compared to that of classical asymmetric septal HCM. AHCM has been classified as pure and mixed types, based on the extent of myocardial involvement. Mixed-type AHCM-which involves the myocardium from the apex to the interventricular septum-is supposed to have poor prognosis compared to pure AHCM; however, there is no definite data to support this.5)
Symptoms of angina are a major clinical manifestation of many variants of HCM, including HCM with ventricular hypertrophy, myocardial bridging, and compression. A previous study revealed that coronary artery disease (CAD) diagnosed by coronary angiography is associated with increased mortality in HCM patients. Moreover, CAD with HCM is associated with higher mortality than HCM with normal LV function.15)
Our study aimed to investigate the impact of CAD on the natural course of AHCM. We also analyzed the general clinical course of AHCM and evaluated other risk factors for cardiovascular (CV) events and the clinical impact of the subtypes of AHCM.
Subjects and Methods
Patients
We enrolled 98 consecutive patients with AHCM 30 years and older who underwent coronary angiography or coronary computed tomography (CT) scans in Yonsei Cardiovascular Hospital and Eulji General Hospital (Korea) between January 2002 and March 2012. AHCM was diagnosed based on two-dimensional (2D) echocardiography. The diagnostic criteria of AHCM was LV hypertrophy which was mainly confined to the apex with wall thickness ≥15 mm and ratio of maximal apical thickness to posterior wall ≥1.5. A complete medical history of all patients was recorded, including diabetes, hypertension, smoking history, atrial fibrillation, previous cerebrovascular accidents, the presence and severity of symptoms such as angina and dyspnea, and medication for any of these conditions.
Two-dimensional and Doppler echocardiography was used to assess left atrial diameter, LV end-systolic and end-diastolic dimensions, LV wall thickness, and presence of obstruction in the intraventricular space or LV outflow tract. Classification as to pure or mixed type was done in 90/98 patients. In the remaining 8/98 patients, classification was unavailable due to a lack of echocardiographic imaging record. The pure type was defined as hypertrophy limited to the apical portion of the LV below the papillary muscle level, whereas the mixed type was defined as apical hypertrophy with coexistent hypertrophy in other LV segments. For AHCM in the "mixed" type, the greatest wall thickness had to be located in the apical segments.5)
Significant CAD was defined as presence of luminal narrowing >50% in at least one vessel of the coronary arteries. Apart from the diagnosis of CAD, the dominancy, blood supply to the apex, and presence of myocardial bridging (only in coronary angiography) were recorded.
This study was approved by the International Review Board at Eulji Hospital.
Clinical follow-up
Using chart reviews, past clinical history, including CV risk factors, was assessed for all the patients. The index of clinical outcome was adverse CV events, including death, non-fatal myocardial infarction or stroke, heart failure (HF), coronary artery revascularization, and hospital admission due to CV disease.
Statistical analysis
All values were expressed as mean±standard deviation. Patients were grouped according to the degree of CAD (absent CAD vs. CAD) and the type of AHCM (pure vs. mixed). We compared continuous variations with independent t-test and categorical variables by Pearson's chi-square test. Differences in the duration of CV event-free survival were evaluated using the Kaplan-Meier survival analysis (log rank test) and Cox proportional-hazards regression model.
All statistical analyses were performed with Statistical Package for the Social Sciences (SPSS) version 18.0 (SPSS Inc., Chicago, IL, USA). P<0.05 was considered statistically significant.
Results
Baseline characteristics
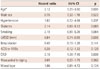
Overall, 98 patients were enrolled in this study. The mean age at the time of enrollment was 61.45±9.78 years, and 38.6% of the patients were female. The proportions of mixed and pure types of AHCM were 34.4% (n=31) and 65.6% (n=59), respectively. In eight patients, discrimination of AHCM type was impossible. The prevalence of hypertension, diabetes, and smoking were 62.2%, 25.5%, and 37.8%, respectively. Beta-blockers and calcium-channel blockers (CCB) were prescribed for 45.9% and 30.6% of patients, respectively. Overall, 74.5% of patients were symptomatic, with chest discomfort (57.1%) being the most common symptom (Table 1).
Coronary angiography and CT scans were performed in 72.4% (n=71) and 27.6% (n=27) of patients, respectively. Significant CAD was found in 31 (31.6%) patients (1-, 2-, 3-vessel disease, and left main disease in 15.3%, 9.2%, 6.1%, and 1.0%, respectively). Myocardial bridging was found in 20.4% (n=20/71) of patients. In the 27 patients who underwent CT scans, determining of myocardial bridging was impossible.
Clinical follow-up data
The mean follow-up period was 53.1±60.7 (median 45.6) months, and CV events occurred in 22.4% (22/98) patients. Mortality occurred in five (5.1%) patients; the cause of death was HF in two cases and cancer in one case. In two cases we could not find the definite cause of death because it occurred outside of the study hospital, but the patients had already been diagnosed as having the CV event (myocardial infarction, revascularization) 14-15 months earlier (Table 2). The patients with CV events were older than those without CV events (mean age, 66.8±7.5 years vs. 59.9±9.9 years). Further, in the CV event group, the smoking rate and LV ejection fraction were higher and the LV end systolic diameter (LVESD) was smaller. Prevalence of mixed-type AHCM was higher in the CV event group, although this difference was not statistically significant (mixed vs. pure AHCM, 50% vs. 30%, p=0.097). Prescription rates of drugs acting on the sympatho-renal axis, such as beta-blockers, angiotensin converting enzyme (ACE) inhibitors, and angiotensin II receptor blockers (ARB) reduced the prevalence of CV events (Table 3). CV events were more frequent in patients with CAD, being more apparent in patients with multi-vessel disease. Myocardial bridging, dominancy, and difference in blood supply to the apex did not affect the clinical outcome (Table 4). At baseline, 12 (12.2%) patients had atrial fibrillation, and during the follow-up period, new onset atrial fibrillation occurred in 10 (10.0%) patients. There was no significant difference in the prevalence of new onset atrial fibrillation according to the presence of CAD {CAD- 11.9% (n=8) vs. CAD+ 6.5% (n=2), p=0.497}.
Comparison of cardiovascular event-free survival
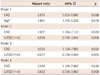
In Cox univariate regression analysis, the CV event-free survival rate was significantly worse in the CAD group {hazard ratio (HR)= 3.18, 95% confidence interval (CI): 1.36-7.45, p=0.008}. Higher age (HR=2.12 per 10 years increase, p=0.005) and smaller LV systolic diameter (HR=0.84 with LVESD increase, p=0.006) were related with poorer prognosis. Myocardial bridging did not affect the CV eventfree survival in AHCM patients (HR=0.61, 95% CI: 0.20-1.75, p= 0.362). Pure-type AHCM showed a tendency toward better survival without statistical significance (HR=1.96, 95% CI: 0.81-4.72, p= 0.134) (Table 5).
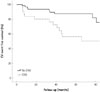
Coronary artery disease persisted as an independent risk factor for CV events (HR=2.91, 95% CI: 1.19-7.13, p=0.021) after adjusting for age and LVESD, which were significantly related with shorter event-free survival in univariate analysis or adding other CV risk factors (Table 6). Kaplan-Meier survival analysis also revealed better survival in patients without CAD {p=0.005 by Log Rank test (Mantel-Cox)} (Fig. 1).
Discussion
Our findings demonstrated CAD diagnosed by coronary angiography or coronary CT scan to be an important risk factor for CV events in AHCM patients, with increasing risk associated with the increasing severity of CAD. Age, smoking, increased LV contractility, and no prescription of beta-blockers, ARB, and/or ACE inhibitors were significantly related to CV events in univariate analysis. Overall, mortality occurred in five patients; however, no cases of definite SCD were observed. AHCM without CAD showed an excellent prognosis even in the advanced age group, with a survival rate of 97.0% and CV event-free survival rate of 86.6% for over 50 months of follow-up. The presence of mixed-type AHCM did not significantly increase the risk of CV events.
Apical hypertrophic cardiomyopathy is a rare disease that occurs only in small proportion of HCM patients. Its natural course is known to be benign; however, some controversial data has been reported in Japanese and western AHCM populations, including the occurrence of SCD and apical aneurysms.5)14)16) Eriksson et al.5) reported the long-term clinical outcomes of AHCM in a comparatively large number of patients (Canada, n=105) for a mean follow-up period of 13.6 years; they demonstrated a low mortality but an increased rate of CV events, including myocardial infarction (10%) and atrial fibrillation (12%), as compared to the general population. Thus, AHCM was shown to have a benign prognosis; however, it was associated with an increased rate of CV events, including 11 cases of myocardial infarction. Unfortunately, this study provided coronary artery anatomical data for only some of the patients (42/105), which were obtained in the course of follow-up.
A previous study concerning HCM (not "AHCM") patients that included the results of coronary angiography, showed that the presence of severe CAD increased mortality rates in these patients.15) Another study reported on coexistent CAD in HCM patients who suffered SCD but did not have the risk factors typically associated with SCD, suggesting that CAD may be an unfavorable prognostic factor in HCM patients.17) To the best of our knowledge, our study is the first to investigate the impact of CAD on the natural course of AHCM with coronary imaging data for all patients. The impact of CAD in AHCM was greater than in HCM, which may be due to the relatively benign clinical course of AHCM. Further, considering the higher mean age of the patients in the present study as compared to that in the previous study (61.45 years vs. 41.4 years), AHCM patients without CAD had a benign natural course that was comparable to the results of the Korean Heart Study which revealed that the 15 year follow-up CV hospitalization rate was 12.6% (54472/430920), and mortality was 2.3% (9943/430920) for 430920 members of the general population aged 30-74 years.18)
Several pathophysiological features of HCM predispose individuals to the development of ischemia, which may be induced by an increased demand for myocardial oxygen or a reduction in the myocardial blood flow and oxygen supply.19) Factors that increase the myocardial oxygen demand include myocyte hypertrophy and increased myocardial mass. Factors that reduce myocardial blood flow include impaired vasodilation and compression of intramural vessels due to myocardial bridging.2)19) Thus, various factors have been proposed to explain ischemia in HCM. As discussed above, the inherent abnormalities of HCM along with the concurrent presence of CAD have a synergistic effect in the induction myocardial ischemia. Therefore, CAD could be an independent prognostic factor by aggravating the inherent ischemic features of AHCM.
In the present study, myocardial bridging was evaluated only in the coronary angiography group; however, it was not observed to affect the natural course of AHCM, similar to a previous study on HCM.20)
Mixed type AHCM, which involves part of LV other than the apex, is supposed to have worse clinical prognosis because of its wider involvement. A previous report showed mixed-type AHCM to be associated with the severity of symptoms but not the clinical outcome.5) The present findings also did not reveal any definitive effects of the AHCM type on the clinical outcomes. Determining the precise extent of myocardial involvement with echocardiography is technically difficult; moreover, in mixed-type AHCM, the extent of involvement is considerably diverse. If magnetic resonance imaging were used to differentiate between pure-type and mixed-type AHCM, the results may differ. However, extensive myocardial involvement apart from the apex does not lead to hemodynamic compromise, such as LV outflow tract obstruction or mitral regurgitation; therefore, it is reasonable that the risk of CV events does not increase significantly in mixed-type AHCM.
Our results revealed that increased LV systolic function and reduced LV end-systolic diameter resulting in advanced hypertrophy were associated with an increased prevalence of CV events. The use of beta-blockers, ACE inhibitors, and ARB-but not CCB-had a protective effect against CV events. These drugs affect the activities of the sympathetic nervous system, suggesting that increased sympathetic nervous activity may adversely affect the prognosis of AHCM. However, in survival analysis, these factors did not significantly affect the event-free survival rate; therefore, the relationship between sympathetic activity and clinical outcomes in AHCM remains unclear.
Limitations
The retrospective nature of this study is a major limitation. As compared to general AHCM patients, the present AHCM cohort was at a comparatively higher risk for CAD and CV events, since coronary imaging studies were not performed randomly, but rather for the evaluation of suspected coronary artery obstructive disease, with 74.5% of the patients being symptomatic and over 50% of the patients reporting chest discomfort. This may have led to a selection bias.
Conclusion
Coronary artery disease diagnosed by coronary angiography or CT scan is one of the most important risk factors for CV events in AHCM patients. AHCM is frequently accompanied by myocardial ischemia and it is associated with a higher CV risk. CAD might aggravate the ischemia of AHCM and lead to worse clinical outcomes. In the absence of CAD, AHCM patients over 30 years of age have a good prognosis, comparable with that of the general population. The benign natural course of AHCM compared to CAD also contributes to the major impact of CAD on AHCM to some degree. To prevent CV events in AHCM with CAD, active CV risk reduction intervention may be needed.




 XML Download
XML Download