

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Kawasaki disease (KD) is an acute systemic vasculitis that was first described in Japan in 1967.1)2) KD is a major cause of acquired heart disease in children in developed countries.3) Many studies have been carried out, but the etiology of KD is still unknown. Infectious, immunologic, and genetic factors seem to contribute to the occurrence of KD.3)4)
The recent consensus is that some infectious agents may trigger an abnormal immune response in children who are genetically susceptible to the disease, leading to acquiring KD.5) The clinical and epidemiologic features of KD could explain the cause of infection. KD predominantly affects children less than 5 years old,6) and children who are 6 months to 2 years old are more vulnerable to KD7) and more susceptible to infection. Boys have a higher incidence of infectious disease8) and KD5)7) than girls.
The incidence of KD is higher in the period between winter and spring when children are often susceptible to numerous respiratory viruses.5)9) Many studies have been carried out to identify infectious agents responsible for KD.4)5)10) However, there is no definitive conclusion regarding this subject.
Respiratory symptoms are frequently observed in children with KD during the acute phase.5)11) Jordan-Villegas et al.12) reported that patients with KD who carry respiratory viruses more frequently showed coronary artery dilatation and were more often diagnosed with incomplete KD. Some studies5)10)12) determined that specific respiratory viruses were associated with KD. However, other authors insisted that the detection of viruses in KD may not have any associative implications.13)
Tissue Doppler imaging (TDI) may be a superior method to measure the Tei index in children because it is less affected by heart rate variability.14) The myocardial performance index (Tei index) evaluates global left ventricle (LV) systolic and diastolic function. It is correlated with severity and clinical outcome in children with cardiac disease.14)
There haven't been any reports about an association between respiratory infection and cardiac function in KD patients.
In this study, we compared laboratory findings in KD patients with febrile patients having a viral infection. Another purpose of this study was to investigate the association of respiratory viruses and cardiac function in children with KD.
Subjects and Methods
Subject
This prospective study was performed on 138 KD patients (80 males, 58 females) at Ewha Womans University Mokdong Hospital from January 2010 to June 2013. We compared 3 groups (group 1: n=94, KD without respiratory symptoms; group 2: n=44, KD with respiratory symptoms; and group 3: n=50, febrile patients with respiratory symptoms). Respiratory symptoms included cough, rhinorrhea, sputum, and sore throat.
To diagnose KD, we used the American Heart Association criteria.15) Diagnosis of the complete type of KD included fever of more than 5 days and at least four of the following: 1) changes in extremities including palm and sole erythema or edema, 2) polymorphous exanthema, 3) bilateral bulbar conjunctival injection without exudates, 4) changes in the lips and oral cavity including erythema, cracked lips, strawberry tongue, and diffuse injection of oral and pharyngeal mucosa, and 5) cervical lymphadenopathy over 1.5 cm in diameter. Children who had a fever lasting 5 or more days and fulfilled two or three principle clinical criteria were regarded as having incomplete KD after other possible causes of fever were excluded.
All KD patients were treated with a single dose of intravenous immunoglobulin (IVIG, 2 g/kg for 10-12 hours) and high dose aspirin (30 mg/kg three times per a day) until having an afebrile status for more than 2 days, after which low dose aspirin (5 mg/kg/day) was administered.
The Ethics committee of Ewha Womans University Mokdong Hospital Institutional Review Board approved this study. Written informed consent was obtained from the parents of all patients.
Laboratory data
Laboratory data obtained from each patient included complete blood count, erythrocyte sedimentation rate (ESR), and levels of alanine aminotransferase (ALT), aspartate aminotransferase (AST), serum total protein, albumin, C-reactive protein (CRP), N-terminal pro-brain natriuretic peptide (NT-proBNP).
Echocardiographic parameters
Echocardiography was performed using an IE33 machine (Philips Medical System, Andover, MA, USA) with an S8 transducer on KD patients and febrile patients who were suspected of having KD during their admission period. Standard parasternal and apical views were acquired. Complete 2D and M-mode echocardiogram, pulsed color-flow Doppler, and TDI were obtained. We measured the following LV parameters by M-mode echocardiography: interventricular septal wall thickness, posterior wall thickness, and LV end diastolic dimension at the chordae tendinae level. Ejection fraction was determined by using the biplane Simpson formula, and fractional shortening was calculated using LV internal dimensions.
The diastolic function was assessed with pulsed Doppler mode from the apical window. Early diastolic velocity (E), late diastolic velocity (A), E/A ratios, and deceleration time were measured using conventional pulsed wave Doppler echocardiography (IE33 machine, Philips Medical System, Andover, MA, USA).
Tissue Doppler imaging
TDI velocities were obtained at the basal septum from the apical four-chamber view. The Doppler beam was aligned as parallel as possible to the direction of the maximum annular motion. TDI was performed to obtain longitudinal myocardial velocity with high quality. A narrow sector angle was used, and image depth was adjusted to allow for a high frame rate (130-160 frames/s) with care taken to avoid angulations. The sweep speed was at least 100 mm/s. The peak systolic myocardial velocity (S'), early diastolic myocardial velocity (E'), and late diastolic myocardial velocity (A') were obtained.
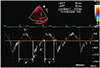
We calculated the Tei index using TDI, which combines systolic and diastolic LV time intervals, using the formula (a-b)/b, where a is the interval between the closing and the opening of the mitral valve, and b is equal to the left ventricle ejection time (LVET) (Fig. 1). Isovolumetric relaxation time (IVRT) was measured from the end of the S' wave to the onset of the E' wave, and isovolumetric contraction time (IVCT) was measured from the end of the A' wave to the onset of the S' wave.
The coronary artery was measured at the parasternal short axis view (Fig. 2). Coronary arteries were defined as abnormal if the internal lumen diameter was greater than 3 mm in children younger than 5 years old,5) if the internal diameter of a segment measured at least 1.5 times that of an adjacent segment, or if the coronary lumen was clearly irregular.16) A giant aneurysm was defined as an internal lumen diameter of greater than 8 mm.17)
Reverse transcription polymerase chain reaction
We collected the nasopharyngeal secretion of KD patients with respiratory symptoms and control febrile patients with respiratory symptoms using nasal and throat swabs on the first day of hospitalization.
Reverse transcriptase-polymerase chain reaction (RT-PCR) was performed using AdvanSure™ RV Real-time PCR (LG Life Sciences, Ltd., Seoul, Korea) using Taqman chemistry technology. This kit performed a primer/probe set with sequences specific to each type of viral pathogen. It performed an analysis of 12 strains of ribonucleic acid (RNA) virus (corona virus 229E/OC43/NL63, parainfluenza virus 1/2/3, influenza A/B virus, respiratory syncytial virus A/B, rhinovirus A/B/C, and metapneumo virus) and 2 strains of deoxyribonucleic acid (DNA) virus (adenovirus and bocavirus). It sequentially performed reverse transcription (RT) and multiple polymerase chain reaction (PCR)s within one PCR tube, and it detected the DNA regions of the bocavirus and the adenovirus. The RNA regions of specific genes of the 12 strains of RNA virus synthesized complementary DNA (cDNA) through RT, then cDNA created each real-time target PCR product along with specific primers. The Taqman probe fluoresced, and fluorescence intensity was measured by the real-time PCR detection system (SLAN-96P Real-time PCR System, Shanghai Hongshi Medical Technology Co., Ltd., Shanghai, China).
Statistical analysis
IBM SPSS Statistics version 18.0 (SPSS Inc., Chicago, IL, USA) was used for all statistic analyses. Data were expressed as mean±standard deviation. Echocardiographic findings were represented as adjusted mean±standard deviation after adjustment for covarients such as CRP and fever duration.
The Kruskal wallis test and the Wilcoxon Rank Sum test were used to compare laboratory data between KD patients and the control group. A p value of less than 0.05 was considered statistically significant.
Results
Comparison of clinical characteristics between groups
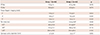
A total of 138 KD patients diagnosed with KD were enrolled in the study. The clinical characteristics of KD patients with and without respiratory symptoms are shown in Table 1. In this study, 94 patients (68.1%) were included in the KD group without respiratory symptoms (group 1), and 44 patients (31.8%) were included in the KD group without respiratory symptoms (group 2). There were no significant differences in age and sex between group 1 and group 2. Fever duration was significantly longer in group 2 than in group 1 (6.2±2.1 days vs. 5.3±1.6 days). In group 2, conjunctival injection was found in 80.9% of the patients, cervical lymphadenopathy over 1.5 cm in 33.0%, skin rash in 71.3%, lip and/or oral mucosal abnormality in 75.5%, palm and/or sole erythema and edema in 62.8%, and Bacillus Calmette-Guérin (BCG) site injection in 29.8% of cases. In group 2, conjunctival injection was found in 72.7% of the patients, cervical lymphadenopathy in 18.2%, skin rash in 52.3%, lip and/or oral mucosal abnormality in 31.8%, palm and/or sole erythema and edema in 22.7%, and BCG site injection in 22.7% of cases. Other features, such as polymorphous skin rash, lip and oral mucosal abnormalities, hand or foot erythema, and edema, were more frequently observed in group 1 (p<0.05), and the rate of incomplete type KD was significantly higher in group 2 than group 1 (61.6% vs. 81.8%, p=0.019) (Table 1).
There were no significant differences in age and sex between group 2 and group 3 (data not shown).
Laboratory data between the Kawasaki disease groups and the control group
There were no significant differences in laboratory tests including those for hemoglobin (Hb), white blood cell count (WBC), percentage of segmented neutrophils (SEG %), platelet count, ESR, CRP, and levels of AST, serum total protein, albumin, and NT-pro BNP between groups 1 and 2. ALT was significantly higher (56.7±84.2 IU/L vs. 93.2±133.7 IU/L) in group 2 compared with group 1.
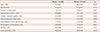
The NT-pro BNP value was higher in group 2 compared with group 3 (698.9±907.7 pg/mL vs. 156.5±112.0 pg/mL, Table 2). Platelet count (301.3±53.4×109/L vs. 239.4±74.9×109/L), CRP (5.9±4.4 mg/dL vs. 3.0±2.8 mg/dL), and ALT (93.2±133.7 IU/L vs. 25.7±43.8 IU/L) were also significantly higher in group 2 than in group 3. Albumin level was significantly lower in group 2 than in group 3 (3.6±0.3 g/dL vs. 4.0±0.3 g/dL). Other laboratory tests including those for Hb, WBC, SEG %, ESR, AST, and total protein showed no significant differences between group 2 and group 3 (Table 2).
Comparison of respiratory viruses between Kawasaki disease patients and the control group
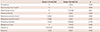
There were no significant differences in positive rates of PCR between group 2 and group 3 (72.7% vs. 78.0%). Group 2 had a higher positive rate for adenovirus than group 3 (54.5% vs. 30.0%, p=0.027). The control group had a significantly higher positive rate for viral PCR for parainfluenza virus 3 (0% vs. 24.0%, p=0.001). For other various viruses including coronavirus, parainfluenza virus (1 and 2), influenza (A and B), respiratory syncytial virus (A and B), rhinovirus (A, B, and C), metapneumo virus, and bocavirus, there were no significant differences in positive rates of respiratory virus PCR (Table 3).
Comparison of Echocardiographic findings between Kawasaki disease patients and the control group
Ejection fraction and fractional shortening were not significantly different between group 1 and group 2. There were no significant differences in late diastolic myocardial velocity (A') (5.6±2.7 cm/s vs. 6.2±2.6 cm/s), early diastolic myocardial velocity (E') (9.9±2.2 cm/s vs. 11.6±6.1 cm/s), systolic myocardial velocity (S') (5.6±1.2 cm/s vs. 6.2±1.4 cm/s), IVRT (41.0±11.7 ms vs. 46.0±12.6 ms), and left LVET (236.4±78.9 ms vs. 210.4±80.2 ms) between group 1 and group 2 (Table 4).
However, IVCT (61.4±8.9 ms vs. 49.5±15.9 ms) and Tei index (0.44±0.06 vs. 0.34±0.07) were significantly higher in group 2 compared with group 1.
Response to intravenous immunoglobulin between Kawasaki disease patients without respiratory symptoms and those with respiratory symptoms
IVIG responders showed improvement in fever and other symptoms after IVIG administration. If KD patients showed fever (higher than 38℃) after 36 hours of IVIG infusion, they were regarded as non-responders, then retreated using a second IVIG.
There were no significant differences in the number of IVIG responders, family history, recurrence, and retreated cases of KD between group 1 and group 2 (Table 5).
Discussion
KD is the most common cause of acquired heart disease among children in developed countries, but the etiology of KD remains unknown. Among many factors that might be associated with KD, infections are considered to be one of the predisposing factors of KD.5)
Burns et al.18) reported significant and consistent seasonal variations in KD patients with a higher incidence in winter and a lower incidence in late summer and fall.
In Korea, KD showed the highest incidence in summer and winter and the lowest incidence in February and October.4)16) The monthly fluctuation in the incidence of KD and the detection of viruses suggests the etiologic importance of the precedence of infection in the development of KD.
According to Tsai et al.19) during the acute stage of KD, 61% of family members of KD patients had acute illnesses, and 92% of them had clusters of infectious disease. These results provide more evidence that KD is strongly associated with infectious disease. It appears that some pathogens are a cause of KD, but no specific pathogen has been found to be a definite cause of KD.5)20)21)
Many studies have been carried out to identify the infectious agents responsible for KD.5)10) Chang et al.5) have suggested that several viruses, such as enteroviruses, adenoviruses, rhinoviruses, and coronaviruses, are associated with KD. The KD patients in their studies had significantly higher positive rates for virus isolation and PCR for those viruses compared with the control group (50.4% vs. 16.4%, p<0.001).
Jordan-Villegas et al.12) stated that respiratory symptoms were frequently observed in children with KD during the acute phase. The association rate of KD with antecedent respiratory illness, including rhinovirus, adenovirus, influenza, parainfluenza, and respiratory syncytial virus, has been reported to range from 56.0% to 83.0%.
In our study, adenovirus, respiratory syncytial virus, rhinovirus, and bocavirus were found in KD patients. Group 2 had a higher rate of positive results for adenovirus than group 3 (54.5% vs. 30.0%, p=0.027). The control group had a significantly higher positive rate for parainfluenza virus 3 (0% vs. 24.0%, p=0.001). In this study, we assumed that some viruses were strongly associated with KD occurrence.
The etiology of KD is still being debated, but the evidence suggests the following: 1) monthly clustering and seasonality,18) 2) geographic prevalence, 3) ethnic tendency, 4) a high association between KD and infectious disease, and 5) higher incidence rates among 6-month to 2-year-old children who have low maternal antibodies and are more susceptible to infections in general.22)23)
Chang et al.5) found that heterogeneous infectious agents, such as common viruses, may trigger KD in young children with certain genetic backgrounds or susceptibility.
On the other hand, Kim et al.13) reported that virus detection rates using multiplex RT-PCR were 32.7% in KD patients and 30.8% in the control group. There was no significant association between respiratory viruses and KD.
KD with respiratory viruses is frequently misdiagnosed as a simple viral infection before other symptoms appear, so the diagnosis can be delayed. KD may be misdiagnosed as another febrile disease such as adenoviral infection, measles, rubella, and scarlet fever.9)
According to Ye et al.24) NT-pro BNP had the highest diagnostic value for KD among other factors including cytokines, CRP, and ESR, which were recommended indexes by the American Heart Association. They found that NT-pro BNP is a reliable marker for the diagnosis of KD and the prediction of IVIG treatment effect. Dahdah et al. 25) reported that NT-pro BNP level was significantly higher in incomplete KD groups than in febrile patients (p<0.05). NT-pro BNP was a useful marker for the diagnosis of KD in patients less than 3 months of age.26) Our study demonstrated that NT-pro BNP is a valuable diagnostic tool in differentiating KD from other febrile respiratory diseases. KD patients with respiratory viruses had significantly higher NT-pro BNP values than control febrile patients in this study (698.9±907.7 pg/mL vs. 156.5±112.0 pg/mL, p<0.05) (Table 2).
The clinical manifestations of adenovirus, especially conjunctival injection, throat injection and prolonged fever, are somewhat like those of KD. KD is frequently misdiagnosed as pharyngoconjunctival fever caused by adenovirus because of the clinical similarity of the two diseases,10) so infusion of IVIG may be delayed. Jordan-Villegas et al.12) has shown that 2.4% of KD patients had adenovirus in their respiratory tract, and 5 of 6 KD patients with concomitant adenovirus infection had incomplete KD. Although virus PCR shows higher sensitivity and detects a relatively low level of virus, viral quantification was not done in this study.
Jordan-Villegas et al.12) found that children with KD who had respiratory virus infections had a higher incidence of coronary artery dilatation than KD patients without viral infections, and the former group were more often diagnosed with incomplete KD. According to Vijayan et al.27) coronary artery dilatation was more frequently observed in incomplete KD than in classical KD (91.7% vs. 41.1%, p<0.001). These findings were similar with our study. Fever duration was significantly longer, and coronary artery diameter was larger in group 2 than in group 1. The rate of incomplete KD was significantly higher in group 2 compared with group 1.
We could not find other articles studying the relevance of respiratory infection and cardiac function in KD patients.
The Tei index combines the systolic and diastolic functions of ventricles in an index of global myocardial performance.14) It correlates with the severity and clinical outcome in children with cardiac disease.14)28) The Tei index could be used as an accurate tool for estimating myocardial function in KD patients.29) According to Ajami et al.30) after IVIG treatment in KD patients, the Tei index changed from 0.43±0.08 to 0.35±0.06. The Tei index could be used to detect early global myocardial dysfunction when other cardiac function indexes are in the normal range.30)
There are several limitations to our study. First, diagnosis of KD was mostly dependent on clinical manifestations since not every patient had coronary artery dilatation. Also, we could not collect nasopharyngeal swab samples from all KD patients with respiratory symptoms because the respiratory virus PCR test was quite expensive. KD patients with respiratory symptoms whose parents did not agree to have their kids test for virus PCR were excluded in this study. Group 1 patients were assumed not to have concomitant viral infections. RT-PCR results for all KD patients would help identify the relationship between respiratory viruses with echocardiographic findings in KD patients.
Second, adenoviral infection could not be distinguished from KD by laboratory tests. Although there are other ways to diagnose viral infection, including adenovirus, such as by using a virus culture or a neutralized antibody, we only used virus PCR to detect respiratory viruses in this study.
Third, the sample size was relatively small. PCR is a relatively easy way to detect respiratory viruses in children, but in this study, whether a virus coexists with or causes KD cannot be distinguished. Viral culture and the quantification of viral loading could help distinguish whether a specific virus simply coexists with or causes KD.
In conclusion, NT-pro BNP is a valuable diagnostic tool in differentiating KD from other febrile viral respiratory infections. KD patients with respiratory symptoms had a higher Tei index than KD patients without respiratory symptoms, suggesting myocardial dysfunction. Further studies are needed to clarify this relevance.


 XML Download
XML Download