

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Heart failure has been defined as a clinical and pathophysiological syndrome that results from ventricular dysfunction, volume or pressure overload, either alone or in combination.1) In children, it leads to characteristic signs and symptoms such as poor growth, feeding difficulties, respiratory distress, exercise intolerance, and fatigue.1)Heart failure is one of the most important pathophysiological syndromes in industrialized nations in terms of overall mortality, morbidity, and cost. The Korean Heart Failure Registry described 3200 heart failure hospitalizations among twenty-four hospitals from 2004 to 2009.2) Survival four years after hospital admission was only 70%. In the United States, it is currently estimated that greater than five million adults have heart failure with projections reaching greater than eight million by 2030.3) One out of nine death certificates mention heart failure, and the mortality at five-years after the diagnosis of heart failure remains at approximately 50%.4) The costs associated with disease is staggering, with estimates that the total annual cost of heart failure in the United States will be nearly $70 billion by 2030.5) Similar data exist from other European and Asian countries.2)6)7)8)
Epidemiology of Pediatric Heart Failure
Though the etiology of heart failure often differs from that of adults, children are not immune from the burden of heart failure. Massin et al.9) reviewed all cardiac admissions at a tertiary pediatric center in Belgium and found that heart failure occurred in 10% of patients, ranging from 6% of patients with congenital heart disease and 80% for cardiomyopathies. Hospital mortality ranged from 4.7% for children with congenital heart disease to 25.0% for cardiomyopathies. In the United States, there are roughly 14000 hospitalizations annually which approximates eighteen admissions per 100000 children.10) This ranks heart failure among the more common serious acute onset conditions of childhood.11) The majority of these children have some form of congenital heart disease, with about 15% having a cardiomyopathy or myocarditis. The disease carries a substantially increased risk of death with an over twentyfold increased risk of hospital mortality compared to pediatric patients without heart failure. Heart failure is a morbid condition in hospitalized patients with respiratory failure, renal failure, and sepsis occurring in a substantial minority of patients. Moreover, these morbidities are associated with a significant increase in the risk of death (Fig. 1). Additionally, these hospitalizations are lengthy, with the average length of stay being nearly twenty days in 2006, placing a substantial burden on families and society. The median hospital charges per admission were over $70000 in 2009 and this amount does not taken into account of the total cost of care beyond the hospitalization or other costs including missed work by parents.12)
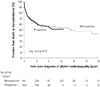
The number of children with chronic heart failure is difficult to ascertain, in part due to the diverse nature of diseases that can lead to heart failure. There are many patients at risk for heart failure from a number of disorders, including congenital heart disease, myocarditis, cardiomyopathy, metabolic disorders, and effects of medications (e.g., anthracyclines). However, not all patients at risk of heart failure will develop heart failure. The incidence of dilated cardiomyopathy form large population-based studies in the United States and Australia range from 0.57 to 0.73 per 100000 children per year.13)14) Not all of these patients will have heart failure at the time of diagnosis, and this number likely underestimates the true incidence as there are likely those with the disease that have not yet been identified. In a prospective study from the United Kingdom, the annual incidence of new-onset heart failure from heart muscle disease was found to be 0.87 per 100000 children who were less sixteen years old.15) Only 66% of these patients were alive or had no transplant one year later.15) This high risk of death or transplant has been confirmed in multiple single center and multi-center reports, with the five-year transplant free survival ranging from 50 to 65% (Fig. 2).16)17)18) The risk for death and transplant is greatest after the initial diagnosis. After one-year, the risk drops significantly with reported events in the range of 1% per year.19) However, not all patients deteriorate, and a significant minority of patients will have a meaningful recovery of ventricular function.20)21) Clearly, further study is needed to understand the worldwide incidence and prevalence of heart failure to understand the true burden of disease and the impact on society.
Diagnosis
For patients with new onset heart failure, the diagnosis can be made form a combination of history, exam findings, laboratory studies, and imaging. Children often present with respiratory and gastrointestinal symptoms, and the severity can range from mild to cardiogenic shock.22) A family history of cardiomyopathy and sudden death may be important clues to a genetic etiology. In addition, to standard laboratory assessment, natriuretic peptides are usually significantly elevated and their trend over time can have important predictive value.23)24) Children that do not have a decrease in their natriuretic peptide levels over time are at increased risk of death, requiring a ventricular assist device (VAD) or needing a heart transplant.
Imaging studies are critical to making the diagnosis of heart failure. Chest X-rays are useful for determination of cardiomegaly and pulmonary edema, though specific cardiac imaging with echocardiogram and/or cardiac MRI is needed. For most forms of cardiomyopathy, the ventricular function will be depressed, though patients with restrictive or hypertrophic cardiomyopathy can have heart failure with preserved ventricular function. While echocardiogram remains the most frequently utilized cardiac imaging modality, cardiac MRI is increasingly becoming utilized. In addition to demonstrating structural abnormalities, ventricular size, and ventricular function, assessments of myocardial inflammation and myocardial scar/fibrosis can be performed.25) These assessments can be useful in determining the etiology of heart muscle disease. Additionally, certain findings, such as diffuse fibrosis as evidenced by T1 mapping, may offer some prognostic information.26) Genetic testing and counseling has also become increasingly important in the diagnosis and management of patients with cardiomyopathy.27)
Medical Therapy
Unlike heart failure therapy in adults, there are few evidencebased data to guide heart failure management in children. There are multiple large prospective multicenter randomized controlled trials in adult heart failure patients with reduced ejection fraction demonstrating the survival advantage of beta-blockers, angiotensin converting enzyme inhibitors, angiotensin receptor blockers, and aldosterone antagonists.28)29)30)31)32) However, many drugs shown to be beneficial in the treatment of heart failure in adults have not been proven to be effective in children.18)33)34)35)36)37)
The reasons for the differences in pediatric and adult studies are not entirely clear and are likely multifactorial.38) It is difficult and expensive to perform high quality prospective studies in pediatric patients with sufficient follow-up and clinically meaningful outcomes. The etiologies of heart failure and comorbid conditions in children and adult are different. As such, the molecular mechanisms, gene expression, microRNA expression, and response to medications may be different in children and adults.39) 40)41)42) Moreover, there are limited data on the pharmacokinetics and pharmacodynamics of heart failure medications in children, and this limited amount of information may lead to inadequate dosing. For example, pharmacokinetics studies of carvedilol suggested that infants and young children may require an increase in the dosing and frequency than was used in the prospective carvedilol trial to achieve a similar serum level to that found to be beneficial in adults.34)43) It should be mentioned, however, that, even though ACEIs and beta-blockers have not clearly been demonstrated to be beneficial for the overall pediatric heart failure population, some etiologies have been shown to respond well to these medications. Kwon et al.44) reported on twenty-three patients with Duchenne and Becker muscular dystrophy from Seoul National University Children's Hospital who were treated with either enalapril or carvediolol. There was an overall improvement in fractional shortening. Additionally, though there were no randomized controlled trials, several other studies have demonstrated a favorable response to these medications in patients with muscular dystrophy.45)46)47)48) Despite convincing trials of the benefits of these medications for most patients with heart failure with reduced ejection fraction, they are widely utilized among pediatric heart failure specialists and recommended by consensus guidelines.1)49)
Likewise, there are few data to provide evidenced-based recommendations for the management of acute heart failure in children. In following the guidelines for heart failure in adults, diuretics and vasodilators are often utilized for patients with symptoms of congestion and adequate perfusion with inotropes reserved for those with impaired perfusion. There are multiple studies in adult heart failure patients that have found increased side effects and mortality among patients treated with inotropes compared to those not treated with inotropes.50)51)52)53) 54) Whether this conclusion is also true among children with heart failure is still unknown. What is known is that inotropes seem to be used in the majority of patients with cardiomyopathy and heart failure admitted to the intensive care unit, and limited data would suggest that the use of these medications are associated with increased mortality.52)54) Further study, however, is needed to determine if it is the disease severity versus the use of inotropes that is associated with adverse outcomes. There are data that suggest the disease severity is greater in children versus adults that are hospitalized with heart failure.55)
Mechanical Circulatory Support
It is arguable that the greatest advance in pediatric heart failure over the last decade has been the increased utilization and success of VADs for patients with end-stage heart failure.56)57) Until relatively recently, the only modality available for small children with profound and refractory hear failure was extracorporeal membrane oxygenation (ECMO). This modality is not ideal for long-term support for heart failure and is one of the strongest risk factors for death while waiting for heart transplantation and for death after transplantation.58)59) The Berlin Heart Excor (Berlin Heart Inc., Woodlands, TX, USA) VAD was first used in the early 1990's in Germany (Fig. 3).60) It was subsequently spread beyond Europe to North America. By the early 2000's, centers in the United States and Canada had gained ample experience with the device and reported good results with a high success rate as a bridge to heart transplantation.56)61) These results led to a prospective multi-center evaluation of the device that compared the VAD to a retrospective cohort of patients treated with ECMO.62) The Excor VAD performed well in the trial with 88-92% patients surviving to heart transplantation or weaning from the device with a favorable neurological outcome (Fig. 4). This result was a significant improvement over ECMO, where there were no patients alive on ECMO after thirty days of support.
While the use of the Excor VAD, in many ways, revolutionized pediatric mechanical circulatory support, there still exists a relatively high adverse side-effect of the device, including a nearly 30% stroke rate.62) Paracorporeal pneumatic pulsatile pumps, like the Excor VAD, have been largely replaced, in adults and older children, by intracorporeal continuous flow VADs, such as the HeartMate II (Thoratec Corp., Pleasanton, CA, USA) and HeartWare HVAD (HeartWare Inc., Framingham, MA, USA) devices.63) These devices in adults have a significantly improved side-effect profile and have allowed many patients to be supported for years with a good quality of life. Limited data in pediatric patients also support the effectiveness of these devices with a favorable side-effect profile.64)65)66)
While many pediatric patients can be well supported with the currently available VADs, there remains certain populations that are still challenging. Small infants with cardiomyopathies still have high adverse events and mortality rate. The National Institutes of Health/National Heart, Lung, and Blood Institute sponsored Pumps for Kids, Infants, and Neonates (PumpKIN) program plans to initiate a trial of the Infant Jarvik VAD in 2015 (Fig. 5).67) Likewise, patients with complex congenital heart disease, including circulatory failure after the Fontan operation, often fare poorly on VADs. As circulatory failure is complex in this population, including the relatively high subset of patients with circulatory failure with relatively preserved ventricular function, a systemic VAD is often inadequate. Limited reports of 'biventricular' support with two VADs or with a total artificial heart suggest patients can be successfully supported to heart transplantation, though further study is needed on the optimal method of support for this population.68)69)
Historically, most of the VAD support in children has been as a bridge to heart transplantation. As the supply of donor organs and organ utilization remain limited in most parts of the world, including the United States and Asia, there are more people with endstage heart failure than available organs for heart transplantation.70)71) Currently in the United States, approximately 40% of VADs in adults are placed as destination therapy, with placement of the VAD having no expectation of a heart transplantation.63) The use of destination therapy increased dramatically after the Randomized Evaluation of Mechanical Assistance for the Treatment of Congestive Heart Failure trial that demonstrated improved survival and quality of life with VAD support in patients with end-stage heart failure that were not eligible for a heart transplantation compared to optimal medical therapy.72) While these indications are still relatively rare in pediatric patients, it has been utilized in certain populations, such as those with Duchenne muscular dystrophy.73) It is likely that use of VADs for patients not eligible for a heart transplantation will continue to grow in the coming years.
Some patients on VADs have meaningful recovery of ventricular function while on support, and some patients have undergone VAD explant and have remained free from heart failure.74) There is mechanical unloading of the ventricle while on VAD support, leading to multiple potential advantageous processes, including decreased wall stress, improved cytoskeletal architecture, improvement neurohormonal profile, and decreased myocardial hypertrophy and death.75)76) Some children have been explanted from VAD due to functional recovery, though most have been in the setting of acute heart failure from myocarditis, graft failure in transplant recipients, or post-cardiotomy heart failure.77)78)79) Given the limitations of heart transplantation, understanding and expansion of VAD utilization as a mechanism for myocardial recovery is of paramount importance in pediatric heart failure.
Conclusion
Heart failure is a common and severe condition that occurs in many children with congenital and acquired heart disease. Though evidence is lacking for much of the medial therapy, many patients can be successfully managed on medications and remain symptom free for a prolonged period of time. A significant proportion of these patients, however, will progress to advanced heart failure, and many will require mechanical circulatory support. There have been tremendous advancements in VAD therapy over the last decade; however, current strategies and devices are often inadequate for small children and those with complex congenital heart disease. Ongoing work is focused on these populations and to expanding the therapy beyond a bridge to heart transplantation into destination therapy and as bridge to recovery.




 XML Download
XML Download