

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Restenosis after coronary angioplasty and graft failure after vascular reconstruction remain unresolved problems for cardiologists and vascular surgeons. One of the major causes of restenosis or graft failure is intimal hyperplasia. However, the precise cellular mechanism of intimal hyperplasia remains unclear.1) Vascular smooth muscle cell (VSMC) proliferation is the normal reactive response after vascular injury. In this process, various types of transcriptional factors are activated and VSMCs migrate from the media across the internal elastic lamina to form a new intimal layer, called the neointima.2) VSMC proliferation contributes to an increase in vessel wall thickness, while decreasing the vascular lumen area.3) The exact mechanism of neointima formation is not fully understood. Many factors may be involved, including growth factors, cytokines, and adhesion molecules,4) which are regulated by nuclear factor-kappa B (NF-κB). NF-κB is a major anti-apoptotic factor, and the aberrant activation of NF-κB is one of the primary causes of a wide range of human diseases, including inflammation, rheumatoid arthritis, asthma, and atherosclerosis.5)6) During NF-κB activation, ubiquitin and the proteasome system play a crucial role. The ubiquitin attaches to the inactive NF-κB complex and I-κBα is degraded by the 26S proteasome.7) After I-κBκ degradation, the activated NF-κB is freed up to translocate to the nucleus and once there it participates in the transcriptional regulation of multiple genes.8)9) Consequently, the proteasome plays a central role in regulating the NF-κB signaling pathway by eliminating I-κBα via protein degradation. Therefore, proteasome inhibitors can exert potent anti-inflammatory and anti-growth promotion actions. Bortezomib is a novel modified dipeptidyl boronic acid that inhibits 26S proteasome-induced I-κBα degradation and suppresses NF-κB activation (Fig.1).10) In this study, using a rat carotid artery injury model, we evaluated the effect of the systemic and local delivery of bortezomib (26S proteasome inhibitor) on reducing neointima formation and restenosis. We also demonstrate that this effect is associated with the inhibition of NF-κB activation and the suppression of I-κBα degradation.
Materials and Methods
Chemical structure of bortezomib
Bortezomib is a modified dipeptidyl boronic acid. The product is provided as a mannitol boronic ester that, in a reconstituted form, consists of mannitol ester in equilibrium with its hydrolysis product, the monomeric boronic acid. The drug substance exists in its cyclic anhydride form as a trimeric boroxine. The chemical name for bortezomib is [(1R)-3-methyl-1-{(2S)-1-15oxo-3-phenyl-2-{(pyrazinylcarbonyl) amino}propyl)amino}butyl] boronic acid, with a molecular weight of 384.24 and its molecular formula is C19H25BN4O4. The solubility of bortezomib, as the monomeric boronic acid, in water is 3.3 to 3.8 mg/mL in the pH range of 2 to 6.5 (Fig. 1).
Animals
Twelve- to fourteen-week-old male Sprague-Dawley rats (Charles River Laboratory, Yokohama, Japan), weighing 300 g each, were fed a normal chow diet and given water ad libitum. All the study protocols were approved by the Chungbuk National University Animal Care and Use Committee.
Balloon angioplasty
The animals were anesthetized with an intraperitoneal injection of ketamine (50 mg/kg) and xylazine (6.7 mg/kg), and the right carotid artery was surgically exposed. The right carotid artery was deendothelialized as described previously.11) Briefly, a Fogarty 2 Fr balloon catheter (Baxter Healthcare Corp., Round Lake, IL, USA) was introduced through the right external carotid artery and advanced into the common carotid artery. The balloon was then inflated with 0.15 mL saline and then withdrawn to the entry point. The entire procedure was repeated three times.
Systemic delivery of bortezomib
In order to evaluate the effect of bortezomib, 0.2 mg/kg of lyophilized bortezomib diluted in sterile 0.9% saline was prepared, and a total volume of 1 mL was administered as a bolus injection via a tail vein immediately after balloon injury (n=10). An identical amount of sterile 0.9% saline was used in the control (balloon injury alone) group (n=10). No additional injection of bortezomib or saline was administered, thereafter.
Perivascular delivery of bortezomib
Immediately after the balloon injury, a local perivascular polymer-based delivery system was used to administer bortezomib to the injured vessel wall in one group of animals (n=4). A separate cohort of animals received an empty gel (n=4). Previous studies from our laboratory and other studies have confirmed that an empty gel has no effect on neointima formation.12) The delivery system consisted of a 40% copolymer gel (F-127; Sigma Chemical Company, Munich, Germany) that contained bortezomib at a concentration level of 4 ug/mL. This was topically applied in a circumferential manner to the exposed adventitia of the carotid artery. F-127 gels exhibit reverse thermal behavior, that is, they remain liquid at refrigerator temperature but become soft gels at body temperature.13)
Western blot analysis
The levels of NF-κB and I-κBα were quantified in the total extracts of whole carotid arteries through western blot analysis, as previously described.21) Briefly, equivalent amounts of protein (20 µg) from each sample were mixed with a gel loading buffer (50 mM Tris, 10% sodium dodecyl sulfate, 10% glycerol, 10% 2-mercaptoethanol, and 2 mg bromophenol blue per mL) at a ratio of 1 : 1. This mixture was boiled for 3 minutes, centrifuged at 10000 rpm for 10 minutes, and then electrophoresed on an 8% discontinuous polyacrylamide minigel. The proteins were transferred onto nitrocellulose membranes, according to the manufacturer's instructions. The membranes were saturated through incubation at 4℃ overnight with 10% non-fat dry milk in phosphate-buffer saline (PBS), and were then incubated with an anti-NF-κB monoclonal antibody or anti-I-κBα (1 : 1000) monoclonal antibody for 2 hours at room temperature. The membranes were washed three times with 1% Triton X-100 in PBS, and then incubated with anti-mouse immunoglobulins coupled to peroxidase (1 : 2000). The immune complexes were visualized using the enhanced chemiluminescence method. Subsequently, the relative expression of the proteins was quantified by the densitometric scanning of the X-ray films, with the scanning, analysis, and calculation performed using the Scion Image System (version 1.01; Scion Corporation, Frederick, MD, USA).
Measurement of In situ vascular smooth muscle cell proliferation
The effect of the perivascular bortezomib treatment (n=3) versus the control (empty gel alone) group (n=3) on In situ VSMC proliferation was measured by bromodeoxyuridine (BrdU) incorporation on day 2 after the injury. Briefly, the perivascular bortezomib-treated rats and control rats were injected subcutaneously with BrdU (30 mg/kg) at 30, 38, and 46 hours after the injury. The carotid artery sections were harvested at 48 hours after the injury and the histological sections were incubated with mouse anti-BrdU monoclonal antibodies (VECTOR, Burlingham, CA, USA). The fraction of BrdU-positive medial VSMC nuclei per cross section was compared between the perivascular bortezomib-treated group and the control (empty gel alone) group.
Histomorphometric analysis
The carotid arteries were perfusion-fixed with 10% buffered formalin. Carotid artery sections (5 µm) were stained with hematoxylin-eosin, and morphometric analysis was performed using 3 individual sections from the middle of each injured arterial segment, by an investigator who was kept blind to the experimental procedure being undertaken. Cross-sectional areas (Aintima and Amedia), the area ratios (Aintima/Amedia), and the percentage area stenosis (% stenosis) were analyzed and calculated using the Scion Image System (version 1.01; Scion Corporation, Frederick, MD, USA).
Immunofluorescence analysis
Immediately following the balloon injury, the carotid arteries were perfusion-fixed with 10% buffered formalin. Carotid artery sections (5 µm) were stained with 4',6-diamidino-2-phenylindole. For immunostaining, the tissue sections were incubated in anti-NF-κB-p65 antibody for 24 hours at 4℃, washed three times in blocking buffer, incubated in an Alexa Fluor 568 anti-rabbit IgG antibody (Molecular Probes, Eugene, USA) for 1 hour, and then analyzed using confocal fluorescence microscopy.
TdT-mediated dUTP nick-end labeling staining
TdT-mediated dUTP nick-end labeling (TUNEL) staining (In Situ Apoptosis Detection kit; Invitrogen, Carlsbad, CA, USA) was employed for the detection of deoxyribonucleic acid fragmentation and apoptotic bodies in rat carotid arteries. Briefly, after deparaffinizing the carotid artery sections (5 µm), digesting protein using proteinase K, and quenching endogenous peroxidase activity with 3.0% H2O2 in PBS, slides were placed in an equilibration buffer, and then, in a working TdT enzyme, followed by a stop/wash buffer. Samples were incubated with TdT in the presence of 11-digoxigenin dUTP at 37℃ for 60 minutes. Samples were then blocked with 2% bovine serum albumin and incubated with antidigoxigenin-peroxidase for 30 minutes at room temperature. After the reaction with diaminobenzidine (Peroxidase Substrate Kit; VECTOR, Burlingham, CA, USA) for 4 minutes, samples were visualized and counterstained with hematoxylin at room temperature for 10 minutes. Samples were evaluated using light microscopy, with apoptotic cells being labeled brown.
Results
Histomophometric analysis in systemic bortezomib treatment
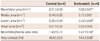
We applied in vivo testing in a rat balloon injury model in order to determine the capability of proteasome inhibition to prevent restenosis. Systemic administration of bortezomib (0.2 mg/kg) resulted in a 29% decrease (0.14±0.03 mm2 vs. 0.10±0.03 mm2, p<0.05) in the neointima area and a 38% decrease (1.68±0.29 vs. 1.05±0.28, p<0.05) in the neointima/media ratio (Fig. 2, Table 1); the dosage administered did not cause mortality.
Histomophometric analysis in perivascular bortezomib treatment
The neointimal area of the bortezomib group was significantly smaller than that of the control group (0.21±0.06 mm2 vs. 0.06±0.01 mm2 p<0.05). The neointima/media area ratio (1.43±0.72 vs. 0.47±0.16, p<0.05) and percentage stenosis (45.5±22.8% vs. 14.5±0.05%, p<0.05) were significantly lower in the bortezomib group (Fig. 3, Table 2). However, the media and vessel wall areas did not differ between the groups, suggesting that any integrity change of the media and negative remodeling did not occur in the bortezomib group.
Measurement of In situ vascular smooth muscle cell proliferation
In vivo medial VSMC proliferation (as assessed by the BrdU proliferation assay) was significantly inhibited in the perivascular bortezomib-treated group at 2 days after the balloon injury (control vs. bortezomib: 24.7±10.9% vs. 10.7±4.7%, p=0.02) (Fig. 4).
Western blot analysis
The expression levels of NF-κB were higher in the control and bortezomib groups compared with the normal carotid artery group. Similar patterns of I-κBα expression were observed in the normal carotid artery and bortezomib groups. A low level of I-κBα expression was detected in the control group at 4 and 12 hours following the balloon injury. Conversely, the NF-κB expression did not differ in the control and bortezomib groups (Supplementary Fig. 1, Online). The bortezomib group exhibited an increased I-κBα expression compared with the control group, suggesting that the inhibition of I-κBα degradation took place in the bortezomib group.
Immunofluorescence analysis
The nuclear import of NF-κB-p65 clearly increased in the control group (n=3) at 1 hour and 4 hours after the balloon injury (Fig. 5, Supplementary Fig. 2, Online). However, the systemic bortezomib treatment group exhibited a clearly decreased nuclear import of NF-κB-p65 at 1 hour and 4 hours after the balloon injury. Similar expression patterns of NF-κB-p65 were observed in the normal carotid artery group (Fig. 5, Supplementary Fig. 2, Online). These results suggest that bortezomib suppressed the nuclear import and activation of NF-κB.
TdT-mediated dUTP nick-end labeling staining analysis
After the balloon injury, the process of cell death was detected at early time points within the innermost area of the media in the control group (n=3) and appeared to radiate in a wave of cell deaths in a time-dependent manner. At 4 hours after the balloon injury, a mass of TUNEL-positive cells (brown in color) was detected in the entire media area. In the bortezomib-treated group (n=3), a few TUNEL-positive cells were detected in the media at early stages and did not change until 4 hours after injury (Supplementary Fig. 3, Online). These findings suggest that bortezomib attenuated massive apoptosis early after vascular injury.
Discussion
Nuclear factor-kappa B is activated by numerous physiological stimuli, and it is commonly associated with immunological and inflammatory processes. In addition, it is also associated with the pathogenesis of proliferative disorders of the vasculature, including atherosclerosis and restenosis.14) After a vascular injury, vascular repair involves four fundamental cellular processes: programmed cell death (apoptosis), cell growth, migration, and matrix modification.15)16) NF-κB is one of the more important transcription factors that initiates the early vascular repair process, contributing to the development of restenosis.9) NF-κB is an inducible transcription factor complex that is composed of a heterodimeric complex, comprising p50 and p65 subunits. In unstimulated cells, NF-κB is held in an inactive form via sequestration in the cytoplasm by the I-κBα family of inhibitor proteins. 14) Phosphorylation of I-κBα typically results in the ubiquination of the protein and subsequent targeting for proteasomal degradation. As I-κBα is degraded, NF-κB is translocated to the nucleus, where it participates in the transcriptional regulation of multiple genes that are involved in the inflammatory process in multiple disease states. By blocking proteasomal activity, I-κBα cannot be degraded and NF-κB remains in the cytosol.8) In our results, western blot analysis showed that the bortezomib group exhibited increased levels of I-κBκ expression at all times compared with the control group. These findings suggest that bortezomib effectively inhibited the proteasomal degradation of I-κBκ. In addition, upon immunofluoresence analysis, the systemic bortezomib treatment group exhibited a clearly decreased nuclear import of NF-κB-p65 compared with the control group at 1 hour and 4 hours after the balloon injury. The systemic bortezomib treatment group exhibited patterns of NF-κB-p65 expression similar to those of the group with normal carotid arteries. Consequently, NF-κB is to be considered an attractive therapeutic target for pharmacologically controlling the vascular response to injury. Therefore, proteasome inhibitors can exert potent anti-inflammatory and anti-proliferative activity by blocking NF-κB activation.
Bortezomib is a cell-permeable dipeptide boronic acid that can reversibly inhibit 26S proteasome, inhibit I-κBα degradation, and suppress NF-κB activation. The reduction of NF-κB activity by bortezomib has been demonstrated as being correlated with antitumor activity in human solid tumors and hematologic malignancies, such as multiple myeloma, lung cancer, breast cancer, and lymphoma.10) Bortezomib is a clinically approved drug and its mechanisms of action, adverse effects, and clinically tolerable dosages are well reported.17) After parenteral injection, bortezomib is both rapidly removed from the vascular compartment and taken up by cells. More than 80% of the injected dosage cannot be detected in plasma after 10 minutes.18) The pharmacodynamic assay reported here indicated that proteasome inhibition occurs in a dose-dependent manner. This inhibition is reversible, and the rate of the return to the baseline (i.e., normal) activity is dose dependent.19) Bortezomib at a dose of 1.3 mg/m2 was administered by intravenous bolus twice weekly in patients with relapsed multiple myeloma.20) The clinical dosage in humans (1.3 mg/m2) is equivalent to 0.15 mg/kg or 1.0 mg/m2 in rats, based on body surface area. In rats, 0.2 mg/kg of bortezomib-induced blood proteasome inhibition was equivalent to that in human clinical trials for cancer treatment.21)22)
It is recognized, nevertheless, that proteasome is an important regulator for normal cellular functioning and cell cycling. Thus, the systemic use of proteasome inhibitors would surely be harmful in use in anti-inflammatory therapy. Furthermore, various cytotoxic side effects, such as gastrointestinal toxicity and hematologic toxicity, as well as cardiovascular side effects, may occur.23) In rats, the safe dose of bortezomib, which does not induce systemic toxicity, is 0.5 to 1.0 mg/kg.24) However, there is no information on how much bortezomib may be required to prevent restenosis.
In our experiment, we used systemic and perivascular bortezomib treatment models in order to evaluate the capacity of proteasome inhibition to prevent restenosis. The rats were treated with 0.2 mg/kg of bortezomib via tail vein injection immediately following carotid balloon injury. This dose produced a 29% decrease in neointima volume at 14 days after the balloon injury. However, although the dose did not cause mortality, hepatosplenomegaly was observed during autopsy procedures. Consequently, in order to reduce neointima formation and to avoid systemic toxicity, we used a lower dose (4 µg/mL) with the perivascular delivery of bortezomib. The dose of 4 µg/mL is approximately 1/15 of that used in systemic cancer treatment. For the perivascular administration of bortezomib, a 40% F-127 solution containing bortezomib (4 µg/mL) was applied immediately following the balloon injury.
In our study, we showed that systemic and perivascular bortezomib treatment groups significantly decreased the neointimal area, neointima/media area ratio, and % area stenosis compared with the control group. However, the systemic treatment group used an anticancer dosage of bortezomib. To minimize the potential systemic side effects, we used preivascular treatment. On BrdU assay performed 2 days after treatment, BrdU-positive cells were significantly decreased in the treatment group. In TUNEL staining analysis, massive apoptosis was detected in the entire media area in the control group. In the bortezomib-treated group, only a low frequency of apoptosis was detected in the media at an early stage. These findings suggest that bortezomib attenuates massive apoptosis in the early stages following a vascular injury. Taken together, it appears that bortezomib inhibited the proteasomal degradation of I-κBα and suppressed the nuclear import of NF-κB. Furthermore, bortezomib reduced early apoptosis, VSMC proliferation, neointimal hyperplasia, and restenosis. These findings indicate that bortezomib has the therapeutic effect of reducing neointmal hyperplasia and inhibiting restenosis after a balloon injury. Furthermore, bortezomib may be a possible candidate drug for the development of a new drug-eluting stent or drug-eluting balloon.
Limitations
The use of proteasome inhibitors has recently been widely investigated in experimental studies and during the treatment of clinical diseases.25)26) However, the safe and effective anti-inflammatory dose of bortezomib remains undetermined. Despite the fact that our study revealed, for the first time, that bortezomib inhibited neointimal formation in a rat carotid artery injury model, further studies are warranted for the following reasons. First, the effective, potent dose of bortezomib was not determined in this study. Second, we did not evaluate any adhesion molecules (i.e., ICAM-1 and VCAM-1), mediators of inflammation (i.e., TNF-a, COX-2, and iNOS), or cytokines (i.e., IL-1, IL-2, and IL-6) that are produced by NF-κB activation. Third, the level of NF-κB needs to be measured by electrophoretic mobility shift assay (EMSA) after nuclear extraction.
Conclusion
Our results demonstrated that the perivascular administration of bortezomib effectively reduced neointima formation after a carotid artery balloon injury in a rat model. Bortezomib inhibited the proteasomal degradation of I-κBα and it suppressed NF-κB activation. Thus, bortezomib represents an attractive drug for attenuating the vascular response after a balloon injury, and it may be useful for the development of a new drug-eluting stent, drug-eluting balloon, and in vascular surgery.





 XML Download
XML Download