

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Thoracic endovascular aortic repair (TEVAR) is increasingly applied in clinical practice as a novel, less invasive treatment for patients with aortic aneurysms and dissection.1) Complications are rare but have become more common as TEVAR has become more popular. Among potential complications, peri-stent graft infection (PGI) is difficult to diagnose but potentially catastrophic. Therefore, early diagnosis and prompt treatment are critical. Here, we report a case of a PGI with secondary aorto-esophageal fistula (AEF) diagnosed by computed tomography (CT) and positron emission tomography (PET) imaging following endovascular treatment of a contained rupture of a pseudoaneurysm of the descending thoracic aorta.
Case
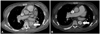
A 50-year-old woman was admitted to the emergency room with back pain, nausea and mild fever for longer than 7 days. Three months prior, she had undergone stent graft implantation with a 28-100 mm SEAL stent graft (S&G, Seoul, Korea) for emergent treatment of a contained rupture of a pseudoaneurysm of the descending thoracic aorta (Fig. 1). The patient had a past history of diabetes mellitus for 20 years and had been on hemodialysis for 16 years. Two months prior, her right leg was amputated below the knee secondary to diabetic foot gangrene. On admission, her temperature was 37.8℃. Laboratory findings were as follows: leukocyte count of 11.47×103/µL with 79.6% neutrophils, hemoglobin of 10.3 g/dL, platelet count of 287×103/µL, erythrocyte sedimentation rate of 120 mm/hr and C-reactive protein (CRP) of 2.29 mg/dL. CT imaging showed the stent graft surrounded by soft tissue and air bubbles in the descending thoracic aorta compared to a previous, immediate post-operative examination (Fig. 2). PGI was suspected based on CT findings. Empirical intravenous vancomycin and tazocin were initiated after obtaining blood cultures but the blood cultures yielded no growth. PET imaging was performed to quantify inflammatory activity and assess the extent of infection. This was notable for increased focal segmental fluorodeoxy-glucose (FDG) uptake around the mid to distal portions of the stent in the descending thoracic aorta (Fig. 2). Although aggressive antibiotic therapy was administered, a mild fever continued. CRP increased from 2.29 to 5.01 mg/dL, and hemoglobin decreased from 10.3 to 8.4 g/dL. Despite the high risk of mortality for performing an operation due to the patient's poor general condition, we decided to perform the surgical removal and aorta repair. A large amount of melena (1.5 L) was passed during induction of general anesthesia. Esophago-gastro-duodenoscopy revealed a 1 cm diameter outpouching in the mid-esophagus which was covered with clotted blood (Fig. 3). Surgical exploration revealed pus-like discharge around the stent graft, with an AEF at the mid third of the esophagus. The infected stent graft was removed and replaced with a Rifampicin-soaked 24 mm Gelweave graft (Terumo, Tokyo, Japan) with primary closure of the AEF. Aorta and vascular graft specimens demonstrated no microorganisms on Gram staining. Despite appropriate intensive care, she died of intractable shock and respiratory failure 9 days after the operation.
Discussion
Aortic PGI and AEF are uncommon but are frequently associated with high mortality and morbidity rates.2) The incidence of PGI ranges between 0.5-5%3) and secondary AEF after TEVAR ranges from 0.5% to 1.7%.4) Prompt diagnosis of these complications is critical due to the high mortality rate, ranging from 20% to 40%.5) It is essential to be suspicious and perform imaging studies, such as CT or PET, without delay in suspected cases, especially in patients with high risk, as the clinical presentation can be non-specific. Risk factors for PGI include immunosuppression, postoperative wound infections, diabetes mellitus, cancer and subsequent invasive procedures.6) Risk factors for AEF include renal dysfunction, pseudoaneurysm and emergent TEVAR.7) The patient with these risk factors is required to be closely monitored because of presented nonspecific symptoms after TEVAR. In our case, the patient had multiple risk factors including diabetes mellitus, chronic renal failure, pseudoaneurysm and emergent TEVAR.
Computed tomography is currently the most commonly used modality for diagnosing PGI, though it can be difficult to distinguish between noninfected and infected grafts on CT.8) As peri-graft air or fluid can be a common postoperative finding during the first 8 weeks following surgery,8) one cannot use these CT findings to definitively identify PGI during this time period following TEVAR. PET scanning can be a complementary imaging modality for diagnosing PGI using the focal FDG uptake pattern as a diagnostic criterion.9) In the current case, the CT scan revealed newly developed, loculated peri-graft air and the PET scan revealed increased FDG uptake around the mid to distal portion of the stent in the descending thoracic aorta, which was felt to most likely represent a peri-graft infection.
Aorto-esophageal fistula can be both a cause and complication of PGI.10) These two disease entities can exist singly or combined. Therefore, if a clinician suspects one of these diseases in a patient, they should consider the possible presence of the other as well.
The two most common treatments for graft infections are conservative treatment with suppressive antibiotic therapy and abscess drainage or a combination of systemic antibiotic therapy11) and surgical removal of the infected graft.12) Of these two, the latter is the superior therapeutic approach. The principle in such surgical treatment is total excision of the infected graft with extra-anatomic bypass.12) In the case of PGI with AEF, extensive aortic reconstruction and adjunctive surgical repair of the esophageal lesion are essential. However, surgical treatment is invasive and is frequently associated with high mortality rates due to these patients' frequently poor overall medical conditions. Surgical endograft removal should be carefully considered based on the clinical and radiologic signs of endograft infection as well as the patient's general condition.
This report highlights midterm complications that occur rarely following thoracic stent graft implantation. As TEVAR becomes more widely used in these complex patients, the operator should be aware of rare, potentially fatal complications such as graft infection or AEF formation after successful implantation of the stent graft.


 XML Download
XML Download