

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Contrast-induced nephropathy (CIN) is usually defined as an acute decline in renal function, expressed as a relative increase in serum creatinine (SCr) concentration of at least 25% or an absolute increase in SCr of 0.5 mg/dL (44.2 µmol/L) in the absence of other etiologies.1) CIN is a significant problem in clinical practice, but also one that is often unrecognized. In 12% of cases, it is the third leading cause of hospital-acquired acute renal failure2) and is associated with 36% mortality in patients who require in-hospital dialysis with 19% survival at 2 years.3)4) When there are no risk factors, the incidence of CIN is low (<5%).5) In modern clinical practice, the characteristic demographic change is a growing elderly population, often patients with cardiovascular and renal comorbidities. Such a change is associated with a greater number of contrast-enhanced invasive diagnostic and interventional coronary procedures, which increases the likelihood of further renal deterioration due to radiocontrast.6)7) In view of the high morbidity and mortality associated with CIN, measures taken to prevent or minimize its occurrence in patients at-risk are extremely important.
Intravascular volume expansion with saline or sodium bicarbonate and low- or iso-osmolar contrast agents, such as iodixanol, are all associated with a decreased rate of CIN.8) Although low- or iso-osmolar contrast agents with adequate hydration reduces the risk for CIN by two-thirds, they did not totally eliminate the risk.9) Therefore, many clinical trials have evaluated various pharmacological agents and periprocedural factors in an effort to identify successful strategies for reducing the risk.10-14) Pharmacological agents evaluated for their potential role in reducing CIN risk include vasodilators and antioxidants, a reflection of the current understanding of the pathophysiology of contrast-induced renal injury. Vasodilatory intervention with dopamine,15) fenoldopam,16) calcium channel blockers,17) and theophylline18) have been investigated, but results are inconsistent, calling for additional large, prospective, randomized studies.
N-acetylcysteine (NAC), a thiol-containing antioxidant, is one of the antioxidants that has been investigated extensively as an agent for CIN prevention.19)20) Tepel and colleagues reported in 2000 an almost 90% relative risk reduction in the incidence of CIN in patients with chronic kidney disease (CKD) given NAC added to prophylactic hydration after intravenous administration of contrast media for elective computed tomography examinations. Moreover, greater efficacy was found with increased NAC dosing (1,200 mg vs. 600 mg, twice daily),21) consistent with the suggestion that the antioxidant effects of NAC are dose-dependent.22) These findings provided the rationale to investigate use of NAC for prevention of CIN in patients with CKD undergoing cardiovascular procedures and receiving intra-arterial contrast agents.
However, despite these positive findings, the true efficacy of NAC for CIN prevention remains unclear given several discordant meta-analyses, mainly as a result of a high degree of heterogeneity among trials.23-29)
Although not having been consistently shown to be effective,30-32) NAC is often recommended and used in an effort to reduce the rate of CIN due to its ease in administration, easy availability, low cost, and few side effects.33)34)
This review focuses on the current status of NAC and intends to guide to renal protection in patients receiving contrast procedures.
N-Acetylcysteine as an Antioxidant-Evidence From Experimental Research
Although there have been a number of in-vivo studies and in vitro animal studies, which have the potential to be extrapolated to humans, the pathogenesis of CIN in humans is still unclear.
The main mechanisms of CIN are suggested as a direct renal tubular toxicity and renal medullary ischemia.35) Administration of contrast medium increases the production of nephrotoxic oxygen free radicals.36)37) There is a large body of evidence that reactive oxygen species have a role in the renal damage caused by radio-contrast agents.38-40)
NAC is an antioxidant that attenuates ischemic renal failure in animal studies.41)42) Besides scavenging oxygen free radicals that mediate cell necrosis after myocardial infarction43) and after angioplasty,44) NAC may act as an antioxidant to inhibit ischemic cell death in the kidney.
Antioxidants such NAC and ascorbic acid protect tubule cells from apoptosis related to reactive oxygen species.45) The cytotoxicity of contrast media (CM) on human embryonic kidney (HEK 293), porcine proximal renal tubular (LLC-PK1), and canine Madin-Darby distal tubular renal (MDCK) cells has been evaluated, and the effectiveness of various antioxidant compounds like NAC, ascorbic acid, and sodium bicarbonate in preventing CM cytotoxicity has been studied. Both low- and iso-osmolar CM induce a dose-dependent renal cell apoptosis. NAC and ascorbic acid, but not sodium bicarbonate, prevents this CM-induced apoptosis.
In a similar study comparing three antioxidants (NAC, ascorbic acid, and probucol), NAC pretreatment significantly improved HEK cell viability as compared with control (p<0.001). Probucol or ascorbic acid pretreatment does not show reduction of cell death caused by CM.46) This result may indicate that NAC is a better antioxidant than ascorbic acid with regard to the CIN prevention.47) The comparison of NAC with ascorbic acid is important, because the combination of these two measures has no additive effect in reducing CIN rate as compared with use of NAC alone.48) This may be mainly attributed to their shared similar mechanism of oxygen free radical scavenging.
A recently published large animal study50) also supports the benefit of NAC in CIN prevention. In the study, intracoronary radiographic CM combined with NAC protected renal function and reduced myocardial infarction size in a pig model of ischemia and reperfusion. Histopathologic analysis of the myocardium revealed a reduction in programmed cell death by NAC-enhanced contrast medium that may explain the increase in ischemia tolerance. NAC-enhanced contrast medium administration blunted the rise in SCr levels by 60% and decreased renal tubule cell apoptosis.
Contrast media also reduce renal function by altering renal hemodynamics as well and NAC has the potential to prevent CIN by improving this. Reduced blood flow in the renal outer medulla, which has a high demand for oxygen and is very vulnerable to hypoxia, might result from increased perivascular hydrostatic pressure, high viscosity, or changes in vasoactive substances such as nitric oxide, adenosine, and endothelin by contrast dye.49)50)
In addition to the CM injected, volume depletion has been recognized as a predisposing factor for CIN. In a study,52) saline or high-osmolar CM was injected into volume-depleted rats and the glomerular filtration rate (GFR) and renal plasma flow rate were measured 24 hours later. Both rates were reduced by 50% in contrast-injected rats, as compared with saline-injected, water depleted rats. CM did not induce renal dysfunction and enhance lipid peroxidation in non-water depleted rats. However in water depleted contrast-treated rats, specific products of membrane lipid peroxidation, namely phosphatidylcholine and phosphatidylethanolamine hydroperoxide, which are markers of oxidative stress, were more than two-fold higher than saline-treated water depleted rats. Therefore, the contrast medium appeared to induce oxidant-mediated injury only in water depleted rats.51)
Some studies have suggested that NAC has vasodilatory properties. In one study with 14 dogs, NAC (150 mg/kg, followed by a 20 mg/kg/hr infusion) increased blood flow in mesenteric, renal and especially femoral arteries than control group.52) Oxygen delivery and oxygen-uptake were higher in the NAC-treated dogs than in the control animals. Moreover, NAC ameliorated ischemia in kidney by general properties as an antioxidant or a possible interaction with NAC and NO.53)
Mitogen activated protein kinases (MAPKs) are integral components of the parallel MAPK cascades activated in response to a variety of cellular stress inducing ischemia/ATP depletion and inflammatory cytokines. Members of the MAPK family, in particular c-Jun N-terminal kinase (JNK), are activated in the kidney following ischemia/reperfusion. Pretreatment with a combination of NAC with sodium nitroprusside and phosphoramidon can completely inhibit MAPK.54) NAC has also been reported to block the expression of vascular-cell adhesion molecule 1 and the activation of nuclear factor-κB in glomerular mesangial cells,55) which implies that NAC may protect kidney function by blocking a signal in the pathogenesis of glomerular mesangial cell disorders.
Clinical Evidence of N-Acetylcysteine
The first human study with respect to kidney function dealt with hepatic failure from drug poisoning. Early administration of NAC prevented a reduction in renal function in patients with acetaminophen poisoning who had liver failure, and NAC may have improved renal function in patients with the hepatorenal syndrome.56-59)
A small clinical study dealing examining NAC in the prevention of CIN was published in 2000.60) The investigators enrolled 83 patients with chronic renal failure (mean SCr, 2.4 mg/dL) who were undergoing computed tomography. NAC (600 mg, orally, twice daily before and after CM) was administered with concomitant saline hydration. CIN occurred 10-times less, 2% in the NAC group and 21% in the control group {p=0.01, relative risk, 0.1; 95% confidence interval (0.02-0.9)}. The publication of these results spurred a myriad of clinical trial, which produced mixed data, even in a meta-analysis.
Patients with acute myocardial infarction treated with primary percutaneous coronary intervention (PCI) are at higher risk of CIN than those undergoing elective PCI.61) In patients with acute myocardial infarction, several conditions may contribute to the development of renal dysfunction. Impaired systemic perfusion due to depressed left ventricular function, a larger dose of contrast medium, and the impossibility of starting renal prophylaxis before exposure to contrast medium may be involved.
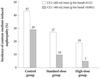
The first study evaluating the effect of NAC on CIN in the setting of primary PCI in patient with ST elevation of myocardial infarction was published in 2006. One hundred and sixteen patients were randomized to receive NAC (600 mg intravenous bolus before CAG and 600 mg orally twice 48 hours after primary PCI), 119 were randomized to receive a double dose of NAC (1,200 mg, same schedule) and 119 were randomized to placebo. SCr increase ≥25% was regarded as confirmation of the development of CIN.62) CIN occurred in a dose responsive manner, with 5% in the double dose NAC group, 15% in the usual dose group, and 33% in the placebo group (p<0.001) (Fig. 1). In-hospital mortality was higher in patients with CIN than those without it (26% vs. 1%, p<0.002). Moreover, the rate for the composite end point of death, acute renal failure requiring temporary renal-replacement therapy, or the need for mechanical ventilation was significantly lower in the double and usual dose NAC groups than placebo, in a dose-dependent manner (5%, 7%, and 17% in the three groups, respectively; p=0.002).
Recently contradictory study results have been published in the same clinical setting with a use of only intravenous NAC in patients with ST-segment elevation myocardial infarction undergoing primary PCI. Activated oxygen protein products and oxidized low-density lipoprotein as markers for oxidative stress were measured with an administration of NAC and placebo. These markers were reduced by as much as 20% in the NAC group (intravenous bolus of 1,200 mg before PCI and 1,200 mg intravenously twice daily for the 48 hours after PCI) (p<0.05), whereas no change was detected in the placebo group. However, the data did not indicate an additional clinical benefit to placebo with respect to CIN. The primary end point, CIN, occurred in 14% of the NAC group and 20% of the placebo group (p=0.28).63)
Another study also demonstrated negative results with intravenous NAC. In the study, 398 acute coronary syndrome patients were randomized to receive an intravenous double dose of NAC (n=205; 1,200 mg bolus followed by 200 mg/hr for 24 hours) and placebo (n=192). There was no difference for the primary end point of CIN defined as an increase in SCr concentration ≥25% above the baseline level within 72 hours of the administration of IV contrast CIN in 16% of the NAC group and in 13% of the placebo group (p=0.40). Recent small-scale studies showed similar negative results.65)
The discrepancy of results may reflect a low contrast dose and, for the negative results, somewhat preserved renal function. Therefore, it is premature to recommend the strategy of intravenous NAC or oral NAC followed by intravenous NAC in primary angioplasty until more definitive data emerges.
Some investigators have argued that NAC influences SCr, the surrogate marker of GFR, without affecting true GFR per se. In an uncontrolled study of healthy volunteers, NAC reduced SCr, but not cystatin C, prompting the conclusion that NAC might affect SCr independent of the GFR.66) However, this effect of NAC has not been investigated in the setting of renal insufficiency. Some contradictory results have been reported. One study that assayed both SCr and cystatin C reported a significant correlation between the parameters at baseline and a stronger correlation 48 hours after contrast exposure in the NAC treatment group.67) Similarly, in randomized trials designed to prevent acute renal deterioration in subjects with renal insufficiency that used peri-operative high-dose NAC infusion (300 mg/kg intravenously), SCr and cystatin C demonstrated concordant response. There was same pattern of creatinine-lowering effect, urinary creatinine excretion and plasma creatinine/plasma cyctatin C ratio for the NAC and placebo groups.68)69) Therefore, it is unlikely that NAC reduced the SCr independent of renal function. It must be noted that the SCr level is an imperfect surrogate outcome measure for nephropathy, and that protection against nephropathy based on altered SCr level has not been confirmed using other measures.
Clinical Researches Not Favoring N-Acetylcysteine Use in Preventing Renal Failure
In a recent large, multicenter, randomized clinical trial including 2,308 patients, coronary angiography was performed in patients with at least one risk factor of CIN (70 years of age, renal failure, diabetes mellitus, full term for HF, hypertension). Patients were allocated to NAC (1,200 mg orally twice daily) before and after the contrast procedure. NAC did not reduce CIN or clinical outcomes. CIN occurred at a same rate, 12.7%, in NAC and placebo groups. Clinical outcomes of mortality or need for dialysis at 30 days was 2.2% and 2.3% in the NAC and placebo group, respectively, with hazard ratio of 0.97 {95% confidence interval (CI), 0.56-1.69; p=0.92} (Table 3).70) In subgroups categorized by basal renal function, contrast dose, age, and diabetes status, there were no differences with respect to CIN rate and cardiovascular events between the NAC and placebo groups.
It is the largest randomized relevant clinical trial performed to date, and was well designed and well conducted. Moreover its statistical power and analysis bring confidence to the results. Considering that the previous conflicting results of small trials and some meta-analyses were rooted in the study heterogeneity and publication bias, where negative results are less likely to be published, this multicenter prospective randomized clinical trial is of great interest and significance. Some expert expressed that this trial will influence clinical practice by dissuading use of NAC for the purpose of renal protection.71)
In light of this latest trial, NAC may well fall out of favor as a routine treatment option until new evidence from studies involving longer duration of use and much higher doses are published. In the interim, a recommendation is to adequately expand intravascular volume with saline at least 12 hours before and after the contrast procedure (Table 1 and 2).
Mixed Results From Some Meta-Analysis
Several meta-analyses were conducted to resolve difficult issue of true effectiveness of NAC. However, the results have been disappointingly equivocal, given the limitations of the small studies on which the analyses were are based.
In 2003, a meta-analysis including seven trials involving 805 patients demonstrated that administration of NAC and hydration significantly reduced the relative risk of contrast nephropathy by 56% {0.435 (95% CI 0.215-0.879), p=0.02} as compared with periprocedural hydration alone in patients with chronic renal insufficiency. However, significant heterogeneity was indicated (overall CIN incidence in NAC group, 2-26%). Other meta-analyses confirmed the heterogeneity in these trials related to publication bias, dose of the agent, cohort studied, and definition of outcome.
Dose may matter. In a recent meta-analysis that included 16 trials involving 1,677 high-risk patients with renal insufficiency using higher NAC doses, a 64% decrease in the likelihood of acute renal failure was evident. This study demonstrated no heterogeneity and no evidence of publication bias (p=0.34). Most studies of NAC's prophylactic potential have used lower doses (e.g., 600 mg twice a day), raising the possibility that the failure to consistently see a benefit may have resulted from under-dosing.
Identified patient and study characteristics may be responsible for some, but not all, of this inconsistency. So, at present, a definitive conclusion cannot be made.
Conclusions
There have been mixed data on whether prophylactic oral and IV NAC administration reduces the incidence of CIN in small trials and even in meta-analyses, although its use is generally recommended, given its low cost, easy availability, and favorable side effect profile. Moreover, evidence of any improvement in clinical outcomes at long-term follow-up is still lacking, despite beneficial effects in CIN prevention.
Research on NAC and the incidence of CIN is too inconsistent at present to warrant a conclusion on efficacy or a recommendation for its routine use. A large, randomized, placebo-controlled trial, a pooled analysis of patient-level data, or both may resolve this issue.
The efficacy of NAC for preventing CIN remains unproven. Future studies should not be based on a primary end point of changed SCr level. Instead, the efficacy and safety of NAC should be sought in critically ill patients at risk for CIN.



 XML Download
XML Download