

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background and Objectives
Subjects and Methods
Results
Conclusion
Figures and Tables
Fig. 1
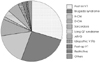
Fig. 2

Fig. 3

Fig. 4

Table 1

Indications for ICD insertion for each patient are listed in this table. In some patients, inducible VT during electrophysiologic study was included as an indication of ICD insertion for primary prevention (This was considered as an indication in previous studies,10) but the relevance of invasively induced arrhythmias appeared to be limited in successive stidies13)). ICD: implantable cardioverter-defibrillator, Pt. No.: the number of patient, SCD: sudden cardiac death survivor, VT: ventricular tachycardia, Family Hx: family history of sudden cardiac death, NSVT: non-sustained ventricular tachycardia during 24 hour Holter monitoring, EPS: ventricular tachycardia induced during electrophysiologic study, EchoCG: excessive LV wall hypertrophy on echocardiography, TMT: abnormal BP response to treadmill test, Second ary: secondary prevention, Primary: primary prevention, ATP: anti-tachycardia pacing setting

Table 3
Ventricular tachyarrhythmias occurred in 6 patients. The types of ventricular tachyarrhythmia and ICD discharge are described in this table. 4 patients received 30 defibrillation shocks and 2 patients received 15 antitachycardia pacings. Except for one case of overdrive acceleration which needed defibrillation shock for termination in patient number 1, all ATPs successfully terminated VTs. ATP setting was not done in patient number 2 due to LV outflow tract obstruction and mitral regurgitation with possible hemodynamic instability during ATP, in patients number 3 and 4 due to presence of fast VT, and in patient number 5 because there had been no previously documented VTs. ICD: implantable cardioverter-defibrillator, Pt. No.: the number of patient, VT: ventricular tachycardia, VF: ventricular fibrillation, ATP: antitachycardia pacing

 XML Download
XML Download