

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Robotic prostatectomy (RP) has been widely performed for treating clinically localized prostate cancer (PC), whereas for treating clinically advanced PC, prostatectomy is usually done by open methods. We evaluated the outcomes of RP for treating patients with clinically advanced PC as compared with the outcomes of RP for treating patients with clinically localized PC.
Materials and Methods
We performed RP in 273 patients with the da Vinci® robot system through a transperitoneal approach. Ninety-two patients had clinically advanced PC (Group I) and 181 patients had clinically localized PC (Group II). We compared the perioperative variables and early surgical outcomes between the two groups.
Results
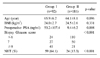
The two groups did not show significant differences for their mean age, but the mean preoperative prostate-specific antigen (PSA) levels and biopsy Gleason scores were significantly higher in Group I. There were no significant differences in the mean operation time (Group I: 214.9±45.1 min, II: 217.8±49.0 min, p=0.709), the estimated blood loss (Group I: 382.8±281.5ml, II: 387.5±369.5ml, p=0.934), the duration of bladder catheterization (Group I: 12.0±2.8 days, II: 12.9±4.6 days, p=0.232), the hospital stay (Group I: 5.9±3.5 days, II: 5.0±2.4 days, p=0.154), and the time to start the postoperative regular diet (Group I: 2.5±1.5 days, II: 2.0±0.6 days, p=0.089) between the two groups. There was a significant difference in lymph node invasion (p<0.001), but no difference in the positive surgical margin (p=0.180). Two out of the 4 intraoperative rectal injuries occurred in the clinically advanced PC group, but they were closed primarily without specific problems, except for 1 case.
Figures and Tables


References
1. Walsh PC, Donker PJ. Impotence following radical prostatectomy: insight into etiology and prevention. J Urol. 1982. 128:492–497.
2. Freedland SJ, Partin AW, Humphreys EB, Mangold LA, Walsh PC. Radical prostatectomy for clinical stage T3a disease. Cancer. 2007. 109:1273–1278.
3. Carver BS, Bianco FJ, Scardino PT, Eastham JA. Long-term outcome following radical prostatectomy in men with clinical stage T3 prostate cancer. J Urol. 2006. 176:564–568.
4. Montie JE. Initial therapy with radical prostatectomy for high risk localized prostate cancer. J Urol. 2006. 176:S27–S29.
5. Ward JF, Slezak JM, Blute ML, Bergstralh EJ, Zincke H. Radical prostatectomy for clinically advanced (cT3) prostate cancer since the advent of prostate-specific antigen testing: 15-year outcome. BJU Int. 2005. 95:751–756.
6. Guillonneau B, el-Fettouh H, Baumert H, Cathelineau X, Doublet JD, Fromont G, et al. Laparoscopic radical prostatectomy: oncological evaluation after 1,000 cases a Montsouris Institute. J Urol. 2003. 169:1261–1266.
7. Bhayani SB, Pavlovich CP, Hsu TS, Sullivan W, Su LM. Prospective comparison of short-term convalescence: laparoscopic radical prostatectomy versus open radical retropubic prostatectomy. Urology. 2003. 61:612–616.
8. Boccon-Gibod L. Radical prostatectomy: open? Laparoscopic? Robotic? Eur Urol. 2006. 49:598–599.
9. Hara I, Kawabata G, Miyake H, Nakamura I, Hara S, Okada H, et al. Comparison of quality of life following laparoscopic and open prostatectomy for prostate cancer. J Urol. 2003. 169:2045–2048.
10. Jaffe J, Stakhovsky O, Cathelineau X, Barret E, Vallancien G, Rozet F. Surgical outcomes for men undergoing laparoscopic radical prostatectomy after transurethral resection of the prostate. J Urol. 2007. 178:483–487.
11. Touijer K, Guillonneau B. Laparoscopic radical prostatectomy: a critical analysis of surgical quality. Eur Urol. 2006. 49:625–632.
12. Menon M, Tewari A, Baize B, Guillonneau B, Vallancien G. Prospective comparison of radical retropubic prostatectomy and robot-assisted anatomic prostatectomy: the Vattikuti Urology Institute experience. Urology. 2002. 60:864–868.
13. Nelson B, Kaufman M, Broughton G, Cookson MS, Chang SS, Herrell SD, et al. Comparison of length of hospital stay between radical retropubic prostatectomy and robotic assisted laparoscopic prostatectomy. J Urol. 2007. 177:929–931.
14. Webster TM, Herrell SD, Chang SS, Cookson MS, Baumgartner RG, Anderson LW, et al. Robotic assisted laparoscopic radical prostatectomy versus retropubic radical prostatectomy: a prospective assessment of postoperative pain. J Urol. 2005. 174:912–914.
15. Tewari A, Srivasatava A, Menon M. A prospective comparison of radical retropubic and robot-assisted prostatectomy: experience in one institution. BJU Int. 2003. 92:205–210.
 XML Download
XML Download