

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Primary aldosteronism is a syndrome characterized by various clinical features that are due to excessive autonomous aldosterone secretion not sustained by the activation of the renin-angiotensin system. Aldosterone-producing adrenal adenoma is found in approximately 35% of the patients who suffer with primary aldosteronism. Laparoscopic adrenalectomy is the standard treatment for aldosterone-producing adrenal adenoma, and the result of this operation is normalization of the serum potassium and plasma aldosterone concentrations, as well as correcting the plasma renin activity in most cases. However, it is known that some of the patients with aldosterone-producing adrenal adenoma show transient hyperkalemia postoperatively due to the reversible suppression of the renin-aldosterone axis. We recently experienced the case of a 54-year-old woman with an aldosterone-producing adrenal adenoma, and she presented with severe hyperkalemia after unilateral adrenalectomy. Compared with the previously reported cases that showed transient suppression of the rennin-aldosterone axis for less than 7 months, our patient revealed a prolonged episode of hyperkalemia for 8 months postoperatively, and this required continuous mineralocorticoid replacement.
Figures and Tables
Fig. 1
Pre-enhanced (A), early-enhanced (B) and delayed-enhanced (C) computed tomographic images of the abdomen. A low density nodular lesion (black arrows) of 1.3 cm diameter is noted on the right adrenal gland. The nodule shows 17 HU on a pre-enhanced scan, 148 HU on an early enhanced scan and 50 HU on a delayed scan with a washout rate of 66%.

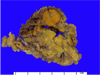
Fig. 2
Gross findings of the surgical specimen. The enlarged globular adrenal gland is seen in fat tissue which measures 1.5 × 1.5 × 1.5 cm. The cut section shows a solitary dark-yellow, oval mass with focal myxoid changes.

References
1. Gordon RD, Ziesak MD, Tunny TJ, Stowasser M, Klemm SA. Evidence that primary aldosteronism may not be uncommon: 12% incidence among antihypertensive drug trial volunteers. Clin Exp Pharmacol Physiol. 1993. 20:296–298.
2. Schirpenbach C, Reincke M. Primary aldosteronism: current knowledge and controversies in Conn's syndrome. Nat Clin Pract Endocrinol Metab. 2007. 3:220–227.
3. Young WF. Primary aldosteronism: renaissance of a syndrome. Clin Endocrinol (Oxf). 2007. 66:607–618.
4. Assalia A, Gagner M. Laparoscopic adrenalectomy. Br J Surg. 2004. 91:1259–1274.
5. Karagiannis A, Tziomalos K, Kakafika AI, Athyros VG, Harsoulis F, Mikhailidis DP. Medical treatment as an alternative to adrenalectomy in patients with aldosterone-producing adenomas. Endocr Relat Cancer. 2008. 15:693–700.
6. Gadallah MF, Kayyas Y, Boules F. Reversible suppression of the renin-aldosterone axis after unilateral adrenalectomy for adrenal adenoma. Am J Kidney Dis. 1998. 32:160–163.
7. Taniguchi R, Koshiyama H, Yamauchi M, Tanaka S, Inoue D, Sato Y, Sugawa A, Muramatsu Y, Sasano H. A case of aldosterone-producing adenoma with severe postoperative hyperkalemia. Tohoku J Exp Med. 1998. 186:215–223.
8. Suh J, Koh G, Park KY, Hong J, Chon S, Oh S, Woo JT, Kim SW, Kim JW, Kim YS. A case of transient hyporeninemic hypoaldosteronism after unilateral adrenalrectomy for aldosterone-producing adenoma. J Korean Soc Endocrinol. 2005. 20:502–506.
9. Tsujihata M, Nonomura N, Tsujimura A, Nishimura K, Yoshimura K, Okuyama A. Laparoscopic adrenalectomy for primary hyperaldosteronism: clinical experience with 60 cases. J Endourol. 2006. 20:262–265.
10. Szücs N, Gláz E, Varga I, Tóth M, Kiss R, Patócs A, Jakab C, Perner F, Járay J, Horányi J, Dabasi G, Molnár F, Major L, Füto L, Rácz K, Tulassay Z. Diagnosis and treatment outcome in primary aldosteronism based on a retrospective analysis of 187 cases. Orv Hetil. 2006. 147:51–59.
11. Gordon RD, Hawkins PG, Hamlet SM, Tunny TJ, Klemm SA, Bachmann AW, Finn WL. Reduced adrenal secretory mass after unilateral adrenalectomy for aldosterone-producing adenoma may explain unexpected incidence of hypotension. J Hypertens suppl. 1989. 7:S210–S211.
12. Ishidoya S, Ito A, Sakai K, Satoh M, Chiba Y, Sato F, Arai Y. Laparoscopic partial versus total adrenalectomy for aldosterone producing adenoma. J Urol. 2005. 174:40–43.
13. Biglieri EG, Slaton PE Jr, Silen WS, Galante M, Forsham PH. Postoperative studies of adrenal function in primary aldosteronism. J Clin Endocrinol Metab. 1966. 26:553–558.
14. Morimoto S, Takeda R, Murakami M. Does prolonged pretreatment with large doses of spironolactone hasten a recovery from juxtaglomerular-adrenal suppression in primary aldosteronism? J Clin Endocrinol Metab. 1970. 31:659–664.
15. Song YW, Lee HK, Min HK. A case of hyporeninemic hypoaldosteronism in diabetes mellitus. J Korean Diabetes Asso. 1981. 6:53–56.
 XML Download
XML Download