

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
Pulmonary hypertension is considered as a poor prognosis factor in patients with chronic obstructive pulmonary disease (COPD). There has been reported brain natriuretic peptide (pro-BNP) is related with increased right ventricular (RV) workloads. However, there are few studies that evaluate the relationship between BNP and pulmonary arterial pressure (PAP), RV function and St. George Respiratory Questionnaire (SGRQ) score in patients with COPD, and the effects of angiotensin converting enzyme inhibitor (ACEI) on these parameters.
Methods
Pulmonary function test, echocardiography, blood BNP, and SGRQ score were evaluated in stabilized moderate degree COPD patients (FEV1/FVC<70%, 50%≤FEV1<80%) aged 45 years and over, without worsening of symptoms within recent 3 months. After treating with ramipril 10 mg for 3 months, the same evaluation was repeated.
Results
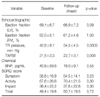
Twenty-two patients were included in this study. BNP was significantly correlated with PAP (Pearson coefficient ρ=0.51, p=0.02), but not with RV ejection fraction (EF) and predicted FEV1%. The values for predicted FEV1% showed significant correlation with SGRQ total score and activity score, but not with BNP or PAP. After ramipril treatment, PAP showed significant decrease (42.8±8.1 vs. 34.5±4.5 mm Hg p=0.0003), tricuspid annular plane systolic excursion significant increase (21.5±3.3 vs. 22.7±3.1 mm p=0.009). BNP showed a tendency to decrease without statistical significance (40.8±59.6 vs. 18.0±9.1 pg/mL p=0.55). SGRQ scores showed no significant change.
Figures and Tables
Figure 1
The relationship between brain natriuretic peptide (BNP) level and pulmonary artery pressure (PAP). BNP was significantly correlated with PAP (p=0.02).
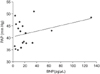
Figure 2
The relationship between FEV1% and St. George Respiratory Questionnaire (SGRQ) total score. FEV1% predicted was significantly correlated with SGRQ total score (SGRQ score=104.3-1.16×FEV1% predicted, p=0.03).

Figure 3
The relationship between FEV1 and brain natriuretic peptide (BNP) levels or pulmonary artery pressure (PAP). There was no significant correlation between FEV1% and BNP level or PAP (sPAP=44.6-0.04×FEV1% predicted, p=0.83; BNP=-26.1+1.5×FEV1% predicted, p=0.28).


References
1. Chaouat A, Bugnet AS, Kadaoui N, Schott R, Enache I, Ducoloné A, et al. Severe pulmonary hypertension and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005. 172:189–194.
2. Hammarström E, Wranne B, Pinto FJ, Puryear J, Popp RL. Tricuspid annular motion. J Am Soc Echocardiogr. 1991. 4:131–139.
3. Kaul S, Tei C, Hopkins JM, Shah PM. Assessment of right ventricular function using two-dimensional echocardiography. Am Heart J. 1984. 107:526–531.
4. Ghio S, Recusani F, Klersy C, Sebastiani R, Laudisa ML, Campana C, et al. Prognostic usefulness of the tricuspid annular plane systolic excursion in patients with congestive heart failure secondary to idiopathic or ischemic dilated cardiomyopathy. Am J Cardiol. 2000. 85:837–842.
5. Passino C, Maria Sironi A, Favilli B, Poletti R, Prontera C, Ripoli A, et al. Right heart overload contributes to cardiac natriuretic hormone elevation in patients with heart failure. Int J Cardiol. 2005. 104:39–45.
6. Mariano-Goulart D, Eberlé MC, Boudousq V, Hejazi-Moughari A, Piot C, Caderas de Kerleau C, et al. Major increase in brain natriuretic peptide indicates right ventricular systolic dysfunction in patients with heart failure. Eur J Heart Fail. 2003. 5:481–488.
7. Troisi F, Greco S, Brunetti ND, Di Biase M. Right heart dysfunction assessed with echography, B-type natriuretic peptide and cardiopulmonary test in patients with chronic heart failure. J Cardiovasc Med (Hagerstown). 2008. 9:672–676.
8. Stein BC, Levin RI. Natriuretic peptides: physiology, therapeutic potential, and risk stratification in ischemic heart disease. Am Heart J. 1998. 135:914–923.
9. Harrison A, Morrison LK, Krishnaswamy P, Kazanegra R, Clopton P, Dao Q, et al. B-type natriuretic peptide predicts future cardiac events in patients presenting to the emergency department with dyspnea. Ann Emerg Med. 2002. 39:131–138.
10. Omland T, Aakvaag A, Vik-Mo H. Plasma cardiac natriuretic peptide determination as a screening test for the detection of patients with mild left ventricular impairment. Heart. 1996. 76:232–237.
11. Mair J, Friedl W, Thomas S, Puschendorf B. Natriuretic peptides in assessment of left-ventricular dysfunction. Scand J Clin Lab Invest Suppl. 1999. 230:132–142.
12. Cheng V, Kazanagra R, Garcia A, Lenert L, Krishnaswamy P, Gardetto N, et al. A rapid bedside test for B-type peptide predicts treatment outcomes in patients admitted for decompensated heart failure: a pilot study. J Am Coll Cardiol. 2001. 37:386–391.
13. Ishii J, Nomura M, Ito M, Naruse H, Mori Y, Wang JH, et al. Plasma concentration of brain natriuretic peptide as a biochemical marker for the evaluation of right ventricular overload and mortality in chronic respiratory disease. Clin Chim Acta. 2000. 301:19–30.
14. Logeart D, Lecuyer L, Thabut G, Tabet JY, Tartière JM, Chavelas C, et al. Biomarker-based strategy for screening right ventricular dysfunction in patients with non-massive pulmonary embolism. Intensive Care Med. 2007. 33:286–292.
15. Turini GA, Brunner HR, Gribic M, Waeber B, Gavras H. Improvement of chronic congestive heart-failure by oral captopril. Lancet. 1979. 1:1213–1215.
16. Cowie MR, Struthers AD, Wood DA, Coats AJ, Thompson SG, Poole-Wilson PA, et al. Value of natriuretic peptides in assessment of patients with possible new heart failure in primary care. Lancet. 1997. 350:1349–1353.
17. Maeda K, Tsutamoto T, Wada A, Hisanaga T, Kinoshita M. Plasma brain natriuretic peptideas a biochemical marker of high left ventricular end-diastolic pressure in patients with symptomatic left ventricular dysfunction. Am Heart J. 1998. 135:825–832.
18. Mair J, Hammerer-Lercher A, Puschendorf B. The impact of cardiac natriuretic peptide determination on the diagnosis and management of heart failure. Clin Chem Lab Med. 2001. 39:571–588.
19. Bettencourt P. NT-proBNP and BNP: biomarkers for heart failure management. Eur J Heart Fail. 2004. 6:359–363.
20. Reesink HJ, Tulevski II, Marcus JT, Boomsma F, Kloek JJ, Vonk Noordegraaf A, et al. Brain natriuretic peptide as noninvasive marker of the severity of right ventricular dysfunction in chronic thromboembolic pulmonary hypertension. Ann Thorac Surg. 2007. 84:537–543.
21. Pieralli F, Olivotto I, Vanni S, Conti A, Camaiti A, Targioni G, et al. Usefulness of bedside testing for brain natriuretic peptide to identify right ventricular dysfunction and outcome in normotensive patients with acute pulmonary embolism. Am J Cardiol. 2006. 97:1386–1390.
22. Inoue Y, Kawayama T, Iwanaga T, Aizawa H. High plasma brain natriuretic peptide levels in stable COPD without pulmonary hypertension or cor pulmonale. Intern Med. 2009. 48:503–512.
23. Kim MA, Kim SH, Zo JH, Hwangbo B, Lee JH, Chung HS. Right heart dysfunction in post-tuberculosis emphysema. Int J Tuberc Lung Dis. 2004. 8:1120–1126.
24. Gemici G, Erdim R, Celiker A, Tokay S, Ones T, Inanir S, et al. B-type natriuretic peptide levels in patients with COPD and normal right ventricular function. Adv Ther. 2008. 25:674–680.
25. King L, Wilkins MR. Natriuretic peptide receptors and the heart. Heart. 2002. 87:314–315.
26. Lang CC, Coutie WJ, Struthers AD, Dhillon DP, Winter JH, Lipworth BJ. Elevated levels of brain natriuretic peptide in acute hypoxaemic chronic obstructive pulmonary disease. Clin Sci (Lond). 1992. 83:529–533.
27. Yetkin O, Hacievliyagil SS, Gunen H. Assessment of B-type natriuretic peptide in patients with pneumonia. Int J Clin Pract. 2008. 62:488–491.
28. He Q, LaPointe MC. Interleukin-1betaregulation of the human brain natriuretic peptide promoter involves Ras-, Rac-, and p38 kinase-dependent pathways in cardiac myocytes. Hypertension. 1999. 33:283–289.
29. Mueller C, Laule-Kilian K, Scholer A, Perruchoud AP. B-type natriuretic peptide for risk stratification in community-acquired pneumonia. J Intern Med. 2005. 258:391–393.
30. Leuchte HH, Baumgartner RA, Nounou ME, Vogeser M, Neurohr C, Trautnitz M, et al. Brain natriuretic peptide is a prognostic parameter in chronic lung disease. Am J Respir Crit Care Med. 2006. 173:744–750.
31. Burke MA, Cotts WG. Interpretation of B-type natriuretic peptide in cardiac disease and other comorbid conditions. Heart Fail Rev. 2007. 12:23–36.
32. Leuchte HH, Holzapfel M, Baumgartner RA, Ding I, Neurohr C, Vogeser M, et al. Clinical significance of brain natriuretic peptide in primary pulmonary hypertension. J Am Coll Cardiol. 2004. 43:764–770.
33. Stolz D, Breidthardt T, Christ-Crain M, Bingisser R, Miedinger D, Leuppi J, et al. Use of B-type natriuretic peptide in the risk stratification of acute exacerbations of COPD. Chest. 2008. 133:1088–1094.
34. Maeder MT, Brutsche MH, Christ A, Reichlin T, Staub D, Noveanu M, et al. Natriuretic peptides for the prediction of severely impaired peak VO2 in patients with lung disease. Respir Med. 2009. 103:1337–1345.
35. Rubin LJ. Cardiovascular effects of vasodilator therapy for pulmonary arterial hypertension. Clin Chest Med. 1983. 4:309–319.
36. The CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure: results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N Engl J Med. 1987. 316:1429–1435.
37. The SOLVD Investigators. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N Engl J Med. 1991. 325:293–302.
38. Di Marco F, Guazzi M, Vicenzi M, Santus P, Cazzola M, Pappalettera M, et al. Effect of enalapril on exercise cardiopulmonary performance in chronic obstructive pulmonary disease: a pilot study. Pulm Pharmacol Ther. 2010. 23:159–164.
39. Mortensen EM, Copeland LA, Pugh MJ, Restrepo MI, de Molina RM, Nakashima B, et al. Impact of statins and ACE inhibitors on mortality after COPD exacerbations. Respir Res. 2009. 10:45.
 XML Download
XML Download