

 ePub
ePub Citation
Citation Print
Print


Abstract
Tuberculosis remains as a major public health problem worldwide. In addition to classic pulmonary tuberculosis, tuberculosis may sometimes present atypically. In the case of atypical tuberculosis, the unusual sites and properties that mimic other diseases can lead to a misdiagnosis and therapeutic delay. Abdominal and pharyngeal tuberculosis are uncommon extrapulmonary manifestations of tuberculosis. To the best of our knowledge, a combination of abdominal and pharyngeal tuberculosis with endobronchial tuberculosis has not been reported. We report a case of concurrent abdominal and pharyngeal tuberculosis in a patient with chronic endobronchial tuberculosis mimicking a metastatic malignancy on computed tomography and FDG-PET.
Figures and Tables
Figure 1
Chest CT scan obtained at admission shows a heterogenous low attenuated mass lesion with calcification(arrow).

Figure 2
Abdomen and pelvic CT scan shows a heterogenous low density mass lesion with calcification(arrow).
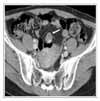
Figure 3
FDG-PET shows hypermetabolic masses at left nasopharynx(arrow), pelvic cavity(arrowhead) and left lower lung(black arrow). Standardized uptake values(SUVs) of nasopharynx, pelvic cavity and left lower lung are 7.1, 4.1 and 3.1, respectively.

Figure 4
Neck CT scan shows rim-enhancing low density lesions at left nasopharyx and oropharynx (black arrow).



References
1. Maher D, Raviglione M. Global epidemiology of tuberculosis. Clin Chest Med. 2005. 26:167–182.
2. Sharma SK, Mohan A. Extrapulmonary tuberculosis. Indian J Med Res. 2004. 120:316–353.
3. Sharma MP, Bhatia V. Abdominal tuberculosis. Indian J Med Res. 2004. 120:305–315.
4. Kim YS, Moon JS, Lee JW, Kim I, Ryu SH, Paik IW. Solitary intra-abdominal tuberculous lymphadenopathy mimicking duodenal GIST. Korean J Intern Med. 2005. 20:72–75.
5. Liu SK, Kim JC, Kim HR, Kim WS, Kim SK. Intestinal and peritoneal tuberculosis : a clinical study of five recent years(1989~1994). Korean J Gastroenterol. 1997. 29:457–464.
6. Al-Serhani AM, Al-Mazrou K. Pharyngeal tuberculosis. Am J Otolaryngol. 2001. 22:236–240.
7. Koktener A. Nasopharyngeal tuberculosis. Eur J Radiol. 2001. 39:186–187.
8. Horsburgh CR, Feldman S, Ridzon R. Practice guidelines for the treatment of tuberculosis. Clin Infect Dis. 2000. 31:633–639.
9. Jeffry L, Kerrou K, Camatte S, Lelievre L, Metzger U, Robin F, et al. Peritoneal tuberculosis revealed by carcinomatosis on CT scan and uptake at FDG-PET. BJOG. 2003. 110:1129–1131.
10. Yoon SJ, Kim PS, Jeong S, Kwon KS, Cho HK, Lee DH, et al. A case of abdominal tuberculosis mimicking cystic mass. Korean J Gastroenterol. 2001. 37:214–217.
11. Kim JH, Lee GG, Hwang HH, Kim YM, Suh JH, Park RJ. Testicular tuberculoss mimicking testicular malignancy. Korean J Urol. 2005. 46:767–769.
12. Chen YK, Shen YY, Kao CH. Abnormal FDG PET imaging in tuberculosis appearing like lymphoma. Clin Nucl Med. 2004. 29:124.
13. Bakheet SM, Powe J, Ezzat A, Rostom A. F-18-FDG uptake in tuberculosis. Clin Nucl Med. 1998. 23:739–742.
14. Chang JM, Lee HJ, Goo JM, Lee HY, Lee JJ, Chung JK, et al. False positive and false negative FDG-PET scans in various thoracic disease. Korean J Radiol. 2006. 7:57–69.
15. Ho CL. Clinical PET imaging-an Asian perspective. Ann Acad Med Singapore. 2004. 33:155–165.
 XML Download
XML Download