

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Post-stroke constipation prevalence rate in stroke patients is 30-60%.1-3 It is difficult to assess constipation objectively, because constipation results in various degrees of subjective symptoms. Therefore, not enough studies are conducted to evaluate this. Constipation not only leads to a low quality of life, but also interferes with rehabilitation treatment because of problems in bowel movement control.4
Post-stroke constipation is caused by inactivity, lethargy, insufficient water or nutrition intake, depression, lack of exercise capabilities, cognitive impairment, reduced consciousness and drug intake. Depending on the changes in the central and peripheral nervous systems, transit time through the small and large intestines can be delayed, and result in incomplete bowel movements.5 In 1989, Wrenn et al.6 reported that fecal impaction is often caused by taking placebo and inactivity in stroke patients with neurological impairments. In 2007, Bracci et al.7 suggested that nitrate and anticoagulants trigger chronic constipation.
Our study aimed to investigate factors affecting bowel movement in acute stroke patients, and measure the correlation between bowel movement and functional recovery.
MATERIALS AND METHODS
Participants
Patients who met the following criteria participated in the study: 1) suffered first acute stroke within a month, 2) admitted to Asan Medical Center, Department of Rehabilitation Medicine from December 2008 to October 2009, 3) scored 24 points or more in the Korean version of Mini - Mental State Examination - Korea (K-MMSE), indicating that the patient was able to inform bowel dysfunction.
Patients with the following characteristics were not eligible for our study: 1) had abdominal surgery in the past, or diseases that could have decreased colonic motility, such as diabetes and hypothyroidism, 2) suffered from gastrointestinal tract disorders in the past, 3) had hernia, congenital large intestine and anal deformity, or colostomy. Patients who met at least two of the following standard rome II criteria8 were in the constipation group: 1) had fewer than three bowel movements a week, 2) strain during at least one of four bowel movements, 3) hard stools at least one of four bowel movements, 4) incomplete bowel movement at least once, 5) feeling of fullness in rectum or anus during at least one of four bowel movements, 6) the need to induce bowel movement with hand at least one of four times.
Methods
Participants' records were used to assess age, sex, parts affected by hemiplegia, National Institutes of Health Stroke Scale (NIHSS), amount of food and water intake, urination volume, accompanying voiding dysfunction or swallowing dysfunction, Adapted Patient Evaluation Conference System (APECS),9 Korean version of Modified Bathel Index (K-MBI), Motricity Index (MI)7 and drug intake.10,11
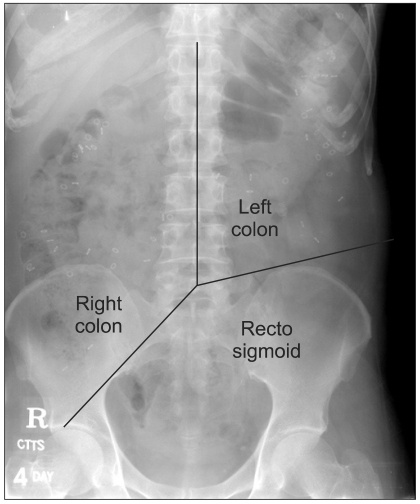
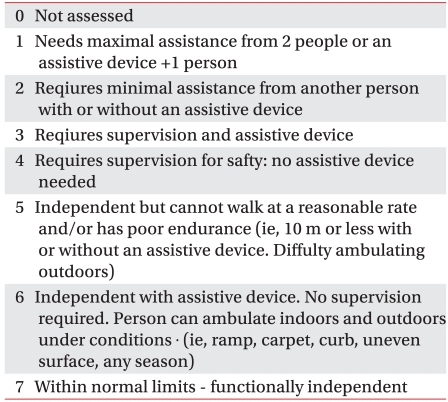
The amount of food intake was recorded every 8 hours for 10 days by the patient or care-givers, and the average amount was then assessed. Patients taking drugs for urinary incontinence, urinary frequency and ischuria were considered as patients with voiding dysfunction. Patients with swallowing disorders were observed for presence of aspiration and/or penetration, using video fluoroscopy, and these patients' food intake was limited. APECS scale was divided into 8 levels (0 to 7), and the responsible therapist and doctor assessed patient walking function using the average level (Table 1). MI was used to measure motor function following stroke, with 100 points referring to normal. In cases of hemiplegia, the average points for the upper and lower extremities of the paralyzed side were measured. While in cases of quadriparesis, the average points for all upper and lower extremities were measured. Colon transit time was measured using Konsyl Phamaceuticals' SITZMARKS® radio-opaque markers, and the procedure by Metcalf et al.12 was used. After the patients were admitted to Asan Medical Center, Department of Rehabilitation Medicine, they stopped taking bowel function enhancement drugs, as well as relaxants and enema. A week later, capsules containing 24 radio-opaque markers were given every morning at 9 am for three days. After four days, plain supine abdominal X-rays were taken. To analyze the X-rays, the pictures were divided into three segments, which were ascending, descending and rectosigmoid colons. The location of the descending colon was defined as the right side of the point where the line connecting the spinous process and the line connecting the L5 and pelvis outlet crosses. The location of the ascending colon was defined as the left side of connecting the L5 and the anterior superior iliac spine. The location of the rectosigmoid colon was defined as below the line connecting L5 and pelvis outlet, and below the anterior superior iliac spine, and the number of radio-opaque markers in each segment was calculated.13 The average transit time was calculated by multiplying the number of radio-opaque markers left in the colon by 1.0 (Fig. 1).14
Both physical therapy and occupational therapy were performed for at least one hour every day, six times a week. After four weeks of rehabilitation, patients were checked for presence of constipation, and the K-MBI was re-evaluated to check for improvements in the activities of daily living function.
Statistical analysis
SPSS version 12.0 (Chicago, IL, USA) was used for statistical analysis. Mann-Whitney U tests were used to compare walking function, activities of daily living function, motor function, level of food and water intake, and colon transit time in the constipation and nonconstipation groups. Chi-Square tests were used to assess presence of constipation, urination disorder and swallowing dysfunction, as well as the effect of the drugs taken. After rehabilitation, Mann-Whitney U tests were also used to compare activities of daily living function in the constipation group and the group of patients with improved conditions.
RESULTS
Participant characteristics
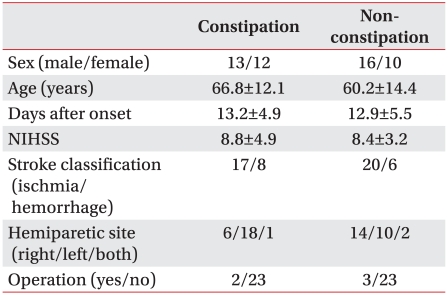
Fifty-one patients, 29 males and 22 females, with a mean age of 63.4±13.6 participated in the study. The patients were divided into two groups, constipation (n=25) and non-constipation (n=26) groups. There were no significant differences between the two groups in sex and onset time of stroke. In addition, there were no significant differences in the patients' National Institute of Health Stroke Scale (NIHSS), parts affected by hemiplegia, and whether they received surgery (Table 2).
Effect of constipation on walking function, daily activities, motor function
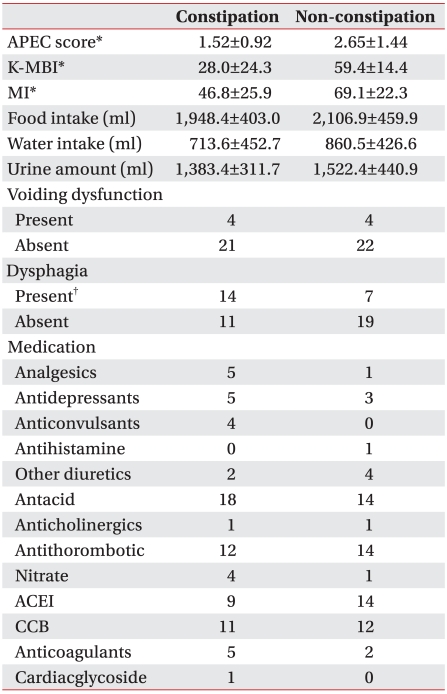
There was a significant difference in walking function when assessed using the APEC scale, the non-constipation group was 2.65±1.44, while the constipation group was 1.52±0.92 (p=0.001). The K-MBI score also showed that the non-constipation group scored 59.4±14.4, while the constipation group scored 28.0±24.3 (p<0.001) (Table 3). The MI score used to assess motor function showed a significant difference as well, in which the non-constipation group scored 69.1±22.3 points and the constipation group scored 46.8±25.9 (p=0.001) (Table 3).
Amount of food and water intake, and constipation
There was no significant difference in the amount of food consumed in the two groups. The non-constipation group consumed 2,106.9±459.9 cc, while the constipation group consumed 1,948.4± 403.0 cc. Water intake was also similar, 860.5±426.6 cc for the non-constipation group, and 713.6±452.7 cc for the constipation group (Table 3).
Effect of voiding function on constipation
Among the participants, 8 patients had voiding dysfunction, 4 each in constipation and non-constipation groups. Therefore, the presence of voiding dysfunction did not have a significant effect on constipation (Table 3). The average amount of urine produced from the two groups showed no significant difference. The non-constipation group produced 1,522.4±440.9 cc, while the constipation group produced 1,383.4±311.7 cc (Table 3).
Effect of swallowing dysfunction on constipation
Twenty-one patients had swallowing dysfunction, 14 of them were in the constipation group, and 7 in the non-constipation group (p=0.048) (Table 3).
Effect of drug intake on constipation
Use of the following drugs had no effect on the presence of constipation (Table 3): Analgesics, antidepressants, antiepileptics, diuretics, antacids, anticholinergics, anticoagulants, nitrates, angiotensin-converting enzyme inhibitors, calcium channel blockers and anticoagulants.
Colon transit time
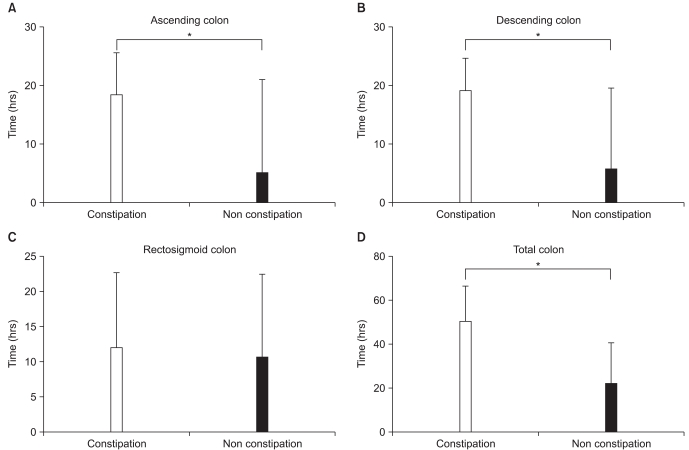
Transit time for the ascending colon in the constipation group was 18.6±15.8 hours, and it was 5.3±7.3 hours (p=0.032) for the non-constipation group. The transit time for the descending colon in the constipation group was 19.3±13.7 hours, whereas it was 5.9±5.5 hours (p=0.029) for the non-constipation group (p=0.029). The transit time for the rectum was 12.3±11.5 hours, and 10.9±10.3 hours for the rectosigmoid colon, while the total transit time was 50.3±18.0 hours, and 22.2±16.4 hours respectively. The difference in the colon transit time between the constipation and non-constipation groups was statistically significant, with the constipation group taking longer (p<0.05) (Fig. 2).
Effect of rehabilitation on improvement in constipation and capacity for day-to-day activities
After four weeks of rehabilitation at Asan Medical Center, Department of Rehabilitation Medicine, 13 out of 51 patients (25.5%) had constipation. Among the 25 patients in the constipation group, 12 people's symptoms improved, and none of the patients from the non-constipation group developed constipation symptoms. The mean K-MBI score of patients with improved symptoms was 17.1±7.9, and the mean K-MBI score of the patients with constipation after four weeks of rehabilitation was 4.8±2.5. The increase in their activities of daily living function was statistically significant in patients with improved symptoms (p=0.002).
DISCUSSION
Constipation is a common complication of stroke, and several studies have been conducted to investigate this. However, compared to voiding dysfunction, not enough research on constipation has been conducted in Korea. Stroke patients often suffer from bowel dysfunction. Bowel problems are used as an indicator of functional recovery limit, and are closely related to the patient and care-givers quality of life.15 In 2009, Su et al.11 reported that constipation in acute stroke patients can be used as an indicator of symptoms to follow 12 weeks after stroke. Constipation in acute stroke patients, therefore, has clinical significance.
In 1975, Lehmann et al.16 reported that compared to the damage in the left cerebral hemisphere, damage to the right hemisphere caused slower recovery. However, In 1986 Jongbloed17 suggested that the damaged part of the brain was irrelevant to the difference in functional recovery. In our study, no significant difference in functional recovery was observed in patients with affected brain regions. In addition, patients were checked for history of surgery, and the presence of constipation according to the affected brain regions, but the results were insignificant. These findings suggest that lesion sites and the patient's history of surgery have no effect on the onset of constipation.
In 1982, Skilbeck et al.18 reported that most patients' walking and bowel function improved within the first three months after stroke, and that walking problems were closely related to bowel functions. Our study also showed that walking function and capacity for day-to-day activities was better in the non-constipation group, and we could assume that is because physical activities affect colon motility.19
Min et al.20 said in 2000 that sufficient amount of food and water intake increased the number of voiding. However, our study showed no significant relationship between the amount of food and water intake and the presence of constipation. A possible explanation is that because only patients admitted to Asan Medical Center participated in our study, all participants' meals were planned, and when patients were consuming insufficient amounts, appropriate measures were taken immediately. Also, voiding dysfunction and the amount of urine did not have significant effects on defecation function in both groups, and this result coincides with what Min et al.20 reported in 2000.
In 2007, Bracci et al.7 reported that the use of antithrombotics and nitrate in stroke patients did not cause constipation. In 2009 Su et al.11 reported that the onset of constipation among patients of stroke using analgesics and diuretics was statistically significant. However, in this study, drug use did not cause constipation.
Although Nino-Mrurica et al.21 in 1990, and Lim et al.22 in 2001 measured colon transit time in patients with spinal cord injury patients, no previous studies had assessed colon transit time in stroke patients. In a study of patients with neurogenic bowel after spinal cord injury, transit time was longer in the descending colon than the ascending colon. While in a study of stroke patients, transit time was considerably longer in ascending and descending colons compared to the rectosigmoid colon.
In 1999, Del Giudice et al.23 reported that in cerebral palsy patients with prolonged colon transit time, most cases were seen in the ascending colon, with 52% of the delay observed in the ascending colon, 36% in the descending colon and 12% in the rectosigmoid colon. In 2004, Park et al.24 showed that transit time was delayed in the proximal colon in cerebral palsy patients with constipation. This study also showed that patients in the constipation group experienced prolonged transit time in the proximal colon, which could have been caused due to neurological problems following lesions.
Our study suggests that the onset of constipation in acute stroke patients and the decline in recovery of function are closely related, since the MBI scores improved significantly in the non-constipation group after four weeks of rehabilitation.
Our study did not include all stroke patients, because patients needed to swallow SITZMARKS® radio-opaque markers to determine colon transit time. Therefore, patients receiving tube feeding were not able to enroll in the study. In addition, patients who scored 24 points or higher in the K-MMSE were able to inform bowel dysfunction and participate in the study. As a result, our study did not fully explain the cause of constipation nor clearly determine the pattern of colon transit time in all stroke patients. The K-MBI scores significantly improved in the non-constipation group, and this could be closely related to the improvement in motor function. However, we did not assess walking function and the MI scores after four weeks of rehabilitation, therefore whether the improvement of motor function enhanced the K-MBI scores remain unclear.
CONCLUSION
Fifty-one acute stroke patients admitted to Asan Medical Center, Department of Rehabilitation Medicine, participated in our study and the conclusions were as follows:
Compared to the non-constipation group, the constipation group had poor walking function and activities of daily living function, as well as weak upper and lower muscles.
More patients in the constipation group suffered from dysphagia, compared to the non-constipation group.
Ascending and descending colon transit time was significantly longer in the constipation group.
A large number of patients in the constipation group no longer suffered from constipation after rehabilitation, and the group with improved symptoms had better activities of daily living function.
When treating acute stroke patients, more attention is needed on bowel dysfunction, and in order to relieve bowel problems, well-planned, comprehensive rehabilitation programs are needed. Further treatment in the constipation group is necessary, since the patients in the group with improved symptoms also had better activities of daily living function.
 XML Download
XML Download