

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Pseudo-Meigs' syndrome is a syndrome that includes hydrothorax and ascites secondary to ovarian tumors other than solid benign fibroma. In this report, we present the case of a 29-years-old female who complained of abdominal distension with peripheral edema during her third trimester. Two solid masses of 15 cm dimension in the left abdomen and 7 cm dimension in the right abdomen were detected by ultrasound and chest X-ray revealed right pleural effusion. Magnetic resonance imaging (MRI) confirmed the ovarian masses and ascites. As the patient had regular uterine contractions, we decided to perform emergency cesarean section because of previous cesarean section history. A laparotomy was performed and pathologists confirmed the presence of a metastatic adenocarcinoma. Four days following the surgery, gastroduodenoscopy revealed a huge ulcerofungating mass was visible in greater curvature of stomach. The final diagnosis was metastatic adenocarcinoma from gastric cancer. Although pseudo-Meigs' syndrome is very rare, it should be carefully considered when evaluating female complaining with ascites in ovarian tumor.
Figures and Tables
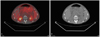
Fig. 1
Trans abdominal ultrasonography shows two huge solid abdominal masses with large amount of ascites.

Fig. 2
Chest X-ray. (A) Chest X-ray on her first hospital visits shows right pleural effusion and subsegmental atelectasis in both basal lungs. (B) After the cesarean section and exploratory laparotomy, chest X-ray shows increased amount of right pleural effusion.
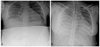
Fig. 3
Gross appearance of the resected bilateral ovarian tumor. (A) A lump of soft mass (11.5×7×3.5 cm, 86 g) in the left ovary and involved fallopian tube. Its surface is yellowish white, solid, and granular with multifocal hemorrhage. (B) Multiple nodules in the right ovary, mesosalpinx and mesovarium with invasion to fallopian tube.

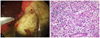
Fig. 4
Gastroduodenoscopy and Biopsy finding. (A) Four days following the surgery, gastroduodenoscopy reveals huge ulcerofungating mass on greater curvature (posterior lower body of the stomach) and edge of ulcer is irregular and unclear. (B) Microscopic examination of the specimen shows that it is poorly differentiated and the mucus remains inside the tumor cell, it pushes the nucleus at the periphery (H&E stain, ×200).

References
1. Meigs JV. Fibroma of the ovary with ascites and hydrothorax; Meigs' syndrome. Am J Obstet Gynecol. 1954. 67:962–985.
2. Ryan RJ. PseudoMeigs syndrome. Associated with metastatic cancer of ovary. N Y State J Med. 1972. 72:727–730.
3. Chen FC, Fink RL, Jolly H. Meigs' syndrome in association with a locally invasive adenocarcinoma of the fallopian tube. Aust N Z J Surg. 1995. 65:761–762.
4. Meigs JV. Pelvic tumors other than fibromas of the ovary with ascites and hydrothorax. Obstet Gynecol. 1954. 3:471–486.
5. Feldman ED, Hughes MS, Stratton P, Schrump DS, Alexander HR Jr. Pseudo-Meigs' syndrome secondary to isolated colorectal metastasis to ovary: a case report and review of the literature. Gynecol Oncol. 2004. 93:248–251.
6. Ayhan A, Tuncer ZS, Bukulmez O. Malignant tumors metastatic to the ovaries. J Surg Oncol. 1995. 60:268–276.
7. Nagakura S, Shirai Y, Hatakeyama K. Pseudo-Meigs' syndrome caused by secondary ovarian tumors from gastrointestinal cancer. A case report and review of the literature. Dig Surg. 2000. 17:418–419.
8. Ohsawa T, Ishida H, Nakada H, Inokuma S, Hashimoto D, Kuroda H, et al. Pseudo-Meigs' syndrome caused by ovarian metastasis from colon cancer: report of a case. Surg Today. 2003. 33:387–391.
9. Wilis RA. Secondary tumors of bones. The Spread of Tumors in the Human Body. 1973. 3rd ed. London: Butterworths;210–227.
10. Hartstein JA, Jacobs AJ, Deppe G, Moshipur J, Cohen CJ. Pseudo-Meigs syndrome with resulting papillary adenocarcinomas of the ovary and fallopian tube. Int J Gynaecol Obstet. 1980. 18:170–171.
11. Kazanov L, Ander DS, Enriquez E, Jaggi FM. Pseudo-Meigs' Syndrome. Am J Emerg Med. 1998. 16:404–405.
12. Terada S, Suzuki N, Uchide K, Akasofu K. Uterine leiomyoma associated with ascites and hydrothorax. Gynecol Obstet Invest. 1992. 33:54–58.
13. Kinmonth JB. Kinmonth JB, editor. Chylous diseases and syndromes, including references to tropical elephantiasis. The Lymphatics: surgery, lymphography and diseases of the chyle and lymph systems. 1982. 2nd ed. London: Edward Arnold;221.
14. Ohtani Y, Ohtani O, Nakatani T. Microanatomy of the rat diaphragm: a scanning electron and confocal laser scanning microscopic study. Arch Histol Cytol. 1993. 56:317–328.
15. Brown RS, Marley JL, Cassoni AM. Pseudo-Meigs' syndrome due to broad ligament leiomyoma: a mimic of metastatic ovarian carcinoma. Clin Oncol (R Coll Radiol). 1998. 10:198–201.
16. Kobayashi F, Sagawa N, Nakamura K, Nonogaki M, Ban C, Fujii S, et al. Mechanism and clinical significance of elevated CA 125 levels in the sera of pregnant women. Am J Obstet Gynecol. 1989. 160:563–566.
17. Gorsse P. Meigs' syndrome and pregnancy. Maroc Med. 1952. 31:907–908.
18. Printer KD. Pseudo-Meigs' syndrome associated with a pregnancy near term. J Obstet Gynaecol Br Commonw. 1967. 74:775–776.
19. Jimerson SD. Pseudo-Meigs's syndrome. An unusual case with analysis of the effusions. Obstet Gynecol. 1973. 42:535–537.
20. Hsu WC, Torng PL, Chow SN, Huang SC. Pseudo-Meigs' syndrome with degenerative uterine leiomyoma in pregnancy. Taiwan J Obstet Gynecol. 2004. 43:161–164.
 XML Download
XML Download