

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Food allergy is an adverse reaction to food mediated by the immunological mechanisms including IgE-mediated, cell-mediated mechanism or both [1]. IgE-mediated food allergy present in 2 different forms: the primary form is due to a sensitization process caused by the ingestion of food allergen. The secondary form results from the sensitization to cross-reactive structure by nonfood allergens which contain homologous part of molecules in the food; i.e., oral allergy syndrome or latex-fruit syndrome [23]. The prevalence of food allergy is increasing in both the pediatric and adult populations [45] resulted in the significant effect on the patient's quality of life. During 2004–2015, the food-related anaphylaxis occupied the second most common cause of the anaphylaxis as 27% in the Emergency Department visit [6]
Fruit and vegetable allergy become more common in the adult. One of the earliest report association between fruit and vegetable allergy with pollen allergy in 1942 [7]. Since then, several fruits are more reported source of allergen by their own properties independently and also their cross-reactivity pattern. Food allergy to fruit is uncertain rate but increase overtime. A systematic review in 2008, 0.4%–6.6% of adults reported adverse reactions to fruits [8].
Bananas are a healthy source of vitamin, mineral and fiber. These fruits being often introduced in the early infant diet. In tropical regions, banana is widely used for numerous purposes, not only for consumption but also added to processed foods as flavourant or ingredient of cosmetics. Banana (Musa acuminata), which belongs to the Musaceae family has been recognized as one of the common fruit allergy for over 50 years [9]. The major and minor allergens in banana have been identified and characterized. Until now, there has been increase number of case report of hypersensitivity reaction to banana average age form infant to elderly and the symptom extended spectrum from mild, local symptom (oral allergy syndrome) to severe systemic reaction [10111213].
Allergic reaction to banana is uncommon. Recent study has been shown prevalence rate 0.04% to 1.2% in general population across the world [14]. Japanese study 2003, allergens related to self-reported anaphylaxis in 319 patients, 2.8% are from bananas [15].
This study aims to determine the clinical characteristics of banana allergy in Thailand and role of allergologic investigations to diagnosis by skin prick test (SPT), prick-to-prick test (PTP), serum specific IgE to banana and food challenge test.
MATERIALS AND METHODS
Approval for the study was obtained from the of Ethics Committee of Mahidol University, Thailand: MURA2018/1038. All patients provided written informed consent.
Six patients who experienced banana hypersensitivity were recruited from adult allergy clinic, Ramathibodi Hospital, Mahidol University between 2015–2018. Demographic data, pattern of banana allergy consisted of the onset of reaction, symptoms, severity, cross-reactivity to kiwi, avocado, latex including type and amount of banana were collected. Atopic history had been explored. The severity of anaphylaxis was classified as Ring and Messmer classification.
SPT with the commercial extract of banana (ALK-Abello Phamaceutical, Inc., Mississauga, ON, Canada) were applied in all patients similar to PTP with the various of banana cultivars (Pisang awake, Cavendish, Silver Bluggoe, Leb-muer-nang, and Khai) and serum specific IgE to banana (ImmunoCAP, Phadia AB, Uppsala, Sweden). Opened-label-banana challenge test with raw and cooked banana was established in all patients except whom experienced ≥ 2 reproducible anaphylactic reaction grade 3 or unconsented patients. The cross-reactivity to kiwi, avocado (using PTP) and latex (using SPT, serum specific IgE to latex (ImmunoCAP) and application test) was evaluated. SPT to common allergen as Dermatophagoides pteronissinus (Der p), Dermatophagoides farina (Der f), Cockroach, Burmuda, Timothy, Johnson grass, Careless weed, and Acacia had been applied.
Regards to SPT, antihistamine was discontinued 10 days before procedure. 0.9% normal saline solution and histamine (ALK-Abello Phamaceutical, Inc.) had been applied as negative and positive control, respectively. Allergens were placed on the volar aspect of the forearm then pricked with 25-G needles. Wheal and flare diameter were evaluated after 15 minutes which positive reaction defined as the mean wheal diameter of 3 mm or greater.
Opened-label banana challenge test (Pisang awak) was established with total 100 g both raw and cooked banana (heating with 200°C for 40 minutes). The protocol started with directed oral contact at inner lip then titrated dose for 5, 15, 30, 50 g, given in 30-minute interval. Positive challenge test was documented when patients developed the reproducible signs and symptoms as the previous history. Standard treatment was prescribed after declared the positive challenge.
RESULTS
Six patients, with the ratio of female:male of 5:1, were enrolled. The median age of onset of banana hypersensitivity was 34 years (interquartile range [IQR], 22–58 years). Anaphylaxis was diagnosed in all patients, 50% presented with anaphylaxis grade III according to Ring and Messmer classification. Skin manifestation as generalized urticaria was the most clinical presentation found in 83.33% (5 of 6 patients) followed by rhinorrhea in 50% (3 of 6 patients). Hypotension was documents in 33.33% (2 of 6 patients) similar to oral pruritus. Dyspnea and diarrhea found in 16.67% (1 of 6 patients) each.
Pisang Awak was the most culprit of banana allergy found in 100% of patients in this study. Fifty percent of the reaction resulted from raw banana similar to heated banana. The median time of the onset of reaction after ingestion was 60 minutes (IQR, 5–150 minutes) with variation in the amount of banana from 1/8 piece to one piece of banana. All of patients experienced at least 2 episodes of banana anaphylaxis before visiting allergy clinic (Table 1).
Table 1
Demographic data and clinical characteristics of banana allergic patients
Positive skin reactivity using commercial banana extract had been documented in 83.33% (5 of 6 patients) with the median diameter of 4.5 mm (IQR, 0–15 mm), sensitivity 83.33% (95% CI, 35.88%–99.58%) while positive skin reactivity (prick-to-prick) using raw Pisang Awak had been found in 100% (6 of 6 patients) with the median diameter of 13.5 mm (IQR, 7–21 mm), sensitivity 100% (95% CI, 54.07%–100%). SPT with different cultivars of banana revealed 100% of cross-reactivities between cultivars (Fig. 1). However, the positive result of serum specific IgE to banana found in 50% (3 of 6 patients), sensitivity 50% (95% CI, 11.81%–88.19%) (Table 2).
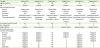
Fig. 1
Prick-to-prick skin test with the various of banana cultivars (Pisang awake, Cavendish, Silver Bluggoe, Leb-muer-nang, and Khai). Skin prick test was also done with kiwi, avocado, and latex allergens.

Table 2
Allergologic investigations for confirmed the diagnosis

B1, Pisang awak (Nam Wa); B2, Cavendish (Hom); B3, Silver Bluggoe (Huk Muk); B4, Leb-muer-nang; B5, Khai; NA, not available.
*Wheal/flare in millimeters. †Ring J, Messmer K. Lancet 1977;1:466-9 [23].
Four of 6 patients had been performed opened-label banana challenge test. Positive banana challenge test revealed in 75% (3 of 4 patients), baked banana in 1 patient and raw banana in 2 patients as shown in Table 2. A case of negative food challenge using baked banana unconsented to test with the raw banana, however she had accidental exposed to raw banana resulted in the anaphylaxis outside the hospital. We did not perform the food challenge test in 2 patients who experienced anaphylactic shock at least 2 episodes.
Cross-reactivity to other fruits and latex was evaluated (Fig. 1). SPT to kiwi and avocado was positive in all patients who applied. According to the clinical history, only 1 patient experienced oral pruritus from kiwi and 1 patient had oral pruritus from kiwi and avocado. However, four of 6 patients ingested these fruits without any reaction. Serum specific IgE for latex found positive result as grades I and II in 66.67% but SPT to latex and application test found negative all (Table 3).
Table 3
Clinical history and Immunologic parameters of cross-reactivities to latex and fruits

Other atopic disease had been documented as allergic rhinitis in 50% (3 of 6 patients) followed by asthma and chronic eczema each in 16.67% (1 of 6 patient). Der p, Der f, and cockroach had been sensitized in 50% (3 of 6 patients) and pollen sensitization found in 33.33% (2 of 6 patients) as shown in Table 1.
DISCUSSION
Banana has been recognized as one of common fruits allergen which manifested in various of the clinical entities as oral allergy syndrome, latex-fruit syndrome and anaphylaxis from banana allergen [161718192021]. The cross reaction IgE antibodies specific for the major birch pollen profilin, Bet v 2, have been shown to cross-react with homologous proteins identified in Banana Mus a1 result in oral allergy syndrome which found frequently in northern European countries [20]. While latex-fruit syndrome caused by N-terminal hevein-like domain of class I chitinase panallergen (Mus a 2) protein shares high homology with Hev b 2 from the rubber tree latex is well-known condition that reported in 30%–70% of latex allergic patients [22]. Banana anaphylaxis without latex allergy also documented in 4-month baby to adult [10111317]. This study reported 6 adult-onset patients who experienced banana anaphylaxis without latex allergy which is the most frequently pattern found in Thailand.
Regards to the allergologic investigation for banana allergy diagnosis in this study, prick-to-prick with raw banana showed the highest sensitivity as 100% (95% CI, 54.07%–100%) followed by SPT with banana commercial extract and serum for specific IgE to banana had the sensitivity as 83.33% (95% CI, 35.88%–99.58%) and 50% (95% CI, 11.81%–88.19%), respectively. High cross-reactivity to other banana cultivars (Cavendish, Silver Bluggoe, Leb-muer-nang, and Khai) was documented as 100%. The sensitization to kiwi and avocado also found as in the previous report [17] however 33.33% (2 of 3 patients) had oral allergy syndrome after ingestion. One of patient (No.3) who experience anaphylaxis grade III from banana had nonreactive skin test to commercial extract as the previous report [19] but had positive skin reactivity to fresh fruit and positive serum specific IgE to banana (Class 3). Patient No.1 showed negative result of serum specific IgE to banana and heated banana challenge test while positive result of SPT and also accidentally anaphylaxis to raw banana (Table 2). The combined test including SPT, serum specific IgE, and food challenge test should be applied for definite diagnosis of banana allergy and component resolved diagnostics might be useful for clinical classification and diagnosis.
The retrospective study design and open-label food challenge test are the weak point in our study but the reciprocal history of anaphylaxis to banana and another method for diagnosis could confirm the true banana allergy.
 XML Download
XML Download