

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Periodontitis, an infectious oral disease caused by specific microorganisms or groups of microorganisms, is characterized by clinical attachment loss, alveolar bone resorption, periodontal pocketing, and gingival inflammation [1]. Microorganisms can cause periodontal tissue destruction in two ways: i) directly by the microorganisms and their degradative products (toxins, lipopolysaccharide, enzymes) and ii) by activation of the host’s immune system, which leads to the recruitment of inflammatory cells, generation of cytokines, release of proteolytic enzymes, and activation of osteoclasts [2]. Thus, periodontal tissue destruction, the characteristic feature of periodontitis, occurs in both host- and microbial-related manners [2]. Microorganisms and their products are the primary etiologic factors that initiate periodontal disease directly; however, the majority of periodontal destruction is caused by host-derived proteolytic enzymes [3]. The primary role of the inflammatory response is to protect the host against microorganisms and their products [3]. Once an inflammatory response has been induced by bacterial stimuli, several tissue-destructive enzymes that are essentially responsible for periodontal tissue destruction have been expressed by various inflammatory cells in periodontal tissues. The purpose of host modulation therapy is to modify or modulate destructive or damaging aspects of the inflammatory host response mediators to those seen in healthy individuals [4].
Matrix metalloproteinases (MMPs) are a family of metal-dependent proteolytic enzymes that degrade the proteinaceous components of the extracellular matrix and cleave signaling proteins [5]. MMPs participate in both physiological (bone remodeling, wound healing, angiogenesis, apoptosis) and pathological (cardiovascular disease, arthritis, cancer, periodontal disease) processes [5]. The regulation of MMP activity occurs through transcriptional regulation of MMP genes, precursor activation, differences in substrate specificity, and MMP inhibitors [5]. Under physiological conditions, there is a balance between MMPs and their inhibitors, called tissue inhibitors of metalloproteinases (TIMPs). TIMPs are specific inhibitors that act by forming an irreversible 1:1 complex with the highly conserved zinc binding site of MMPs [6]. The expression and activity of MMPs are affected by bacterial virulence factors and cytokines in periodontal disease [7]; active MMP levels increase and exceed TIMP levels, thus disturbing the balance between MMPs and TIMPs and shifting the ratio toward MMPs. The imbalance between MMPs and TIMPs in favor of enzymatic activity in periodontal disease leads to degradation of the extracellular matrix and alveolar bone [8]. MMP-1 and -8 belong to the collagenase group of the MMP family, and it has been reported that both MMP-1 and -8, the major interstitial collagenases, degrade the extracellular matrix in periodontal disease; MMP-8 is the predominant form of collagenase in chronic periodontitis and MMP-1 is the main collagenase in localized aggressive periodontitis [9]. Evidence indicates that the amounts of MMP-1 and -8 in gingival crevicular fluid and saliva are elevated during periodontal disease and reduced after periodontal treatment [91011]. In contrast, experimental studies have shown that MMP-8 can also exert a protective and anti-inflammatory role in Porphyromonas gingivalis-induced alveolar bone loss, as demonstrated in MMP-8 knockout mice [1213]. TIMP-2 is a specific inhibitor of MMPs and plays a role not only in MMP inhibition, but also in MMP activation [14]. Elevated TIMP-2 levels have been detected differentially and site-specifically in periodontal inflamed tissue; this marker decreases after periodontal therapy [111516]. In contrast, decreased TIMP-2 levels have been found in tissue extract supernatants and gingival crevicular fluid from periodontitis-affected patients compared with healthy controls [7]. A study by Kubota et al. [8] reported that higher MMP-1/TIMP-2 ratios were observed in periodontitis lesions than in healthy gingival tissue. Thus, it is clear that the balance between MMPs and their inhibitors is critical in the development of disease management strategies.
In recent years, there has been a growing interest in flavonoids and their biological effects [17]. Flavonoids are low-molecular-weight polyphenolic compounds characterized by a diphenylpropane structure that make up a group of plant secondary metabolites with beneficial effects such as antioxidant, anti-inflammatory, antimicrobial, anticancer, cardioprotective, neuroprotective, antidiabetic, antiosteoporotic, estrogenic/antiestrogenic, anxiolytic, analgesic, and antiallergic activities [17]. Kaempferol, one of the most common dietary flavonoids, is found in tea, broccoli, apples, strawberries, and beans [17]. This flavonol has been shown to possess a number of strong biological effects, such as antioxidant, anti-inflammatory, anticarcinogenic, and antiallergic activities [1718]. Kaempferol inhibits nitric oxide production and inducible nitric oxide synthase protein expression in Prevotella intermedia lipopolysaccharide-stimulated RAW264.7 cells via heme oxygenase-1-mediated reactive oxygen species reduction [18]. In light of these observations, the authors hypothesized that kaempferol could be a potent modulator of the host response in periodontal therapy [18].
While MMP-1, MMP-8, and TIMP-2 have been studied in several diseases as well as periodontal disease, no study has until now documented potential effects of kaempferol on these markers in periodontal disease. As periodontitis is an inflammatory and bone-destructive disease, and microbial dental biofilm accumulation is the primary etiological factor for periodontal disease, detection of the effect of kaempferol application may be useful due to its anti-inflammatory effect for periodontal therapy in the presence and absence of microbial dental biofilm.
The aim of this study was to examine, for the first time, the effect of kaempferol application on the periodontium by histomorphometric analysis and on gingival tissue MMP-1, MMP-8, and TIMP-2 levels by biochemical analysis in rats after experimental periodontitis induction with/without the presence of microbial dental biofilm.
MATERIALS AND METHODS
Sixty male Wistar albino rats, each weighing 200 g, were used in this study. The rats were housed separately in plastic cages with controlled room temperature (22±1°C) and humidity (50%), and they were maintained in a 12:12-h light–dark cycle with food and water available ad libitum. All animal care and experimental protocols were in compliance with guidelines approved by the Animal Experiments and Ethics Committee of Ondokuz Mayis University (Protocol No. 2012/18).
Sample size calculations
No sample size calculation could be performed before the study, because there was no precise information available regarding kaempferol effects in experimental periodontitis. We therefore based our estimates on a pilot study, which included 8 rats in each group. The sample size was calculated based on the results of MMP-8 levels between kaempferol-treated groups and their control groups. A sample size of 10 per group was required for detection of a significant difference (80% power, two-sided 5% significance level).
Experimental periodontal disease protocol
The 60 rats were randomly allocated to the following groups: Group 1 (n=10), healthy control; Group 2 (n=10), experimental periodontitis; Group 3 (n=10), systemic saline without ligature; Group 4 (n=10), systemic kaempferol without ligature; Group 5 (n=10), systemic saline with ligature; and Group 6 (n=10), systemic kaempferol with ligature. Experimental periodontitis was induced by tying 3.0 sterile silk ligatures around the cervical area of the right and left mandibular first molars in all groups except Group 1, the healthy control group. This procedure was performed under general anesthesia with ketamine hydrochloride and xylazine. The ligatures were kept in position for 15 days to promote microbial dental plaque accumulation and inflammation [19]. Systemic saline and kaempferol (Sigma-Aldrich, St. Louis, MO, USA) (3,5,7-trihydroxy-2-[4-hydroxyphenyl]-4H-1-benzopyran-4-one) were administered to the rats with experimental periodontitis in two different periods. In Period 1, the ligature was removed after experimental periodontitis induction (15 days), and then kaempferol and saline were administered for ten days. In Period 2, the ligature was kept in position after experimental periodontitis induction (15 days), and then kaempferol and saline were administered for ten days, except in Group 2, the experimental periodontitis group. Kaempferol was administered systemically five times, in doses of 10 mg/kg/day every two days [20]. Systemic application of kaempferol (administered in saline solution) and saline was performed by oral gavage.
All of the rats were euthanized while under general anesthesia at the end of the experimental period. The mandibles were carefully removed along with the surrounding gingiva, and the gingival tissue samples were extracted from the buccal region of the mandibular right first molars.
Histomorphometric analysis
The left side of the mandible removed with the surrounding gingiva was fixed in 10% neutral buffered formalin. The samples were then decalcified in 8% formic acid (14 days) and embedded in paraffin. Serial paraffin sections (5 µm) were made from the mesiodistal aspects throughout the mandibular first molars. Three sections representative of the central area of each tooth were observed and stained with hematoxylin and eosin (H&E).
As described in our previous study [21], the following parameters were assessed in each section stained with H&E: 1) the percentage of alveolar bone in the furcation area; 2) alveolar bone level; and 3) attachment level. The furcation area was determined in the inter-radicular area, which was limited by an imaginary line drawn between the roots (Figure 1A). The percentage of alveolar bone area on each specimen was calculated as the ratio of the alveolar bone area to furcation area (Figure 1B). The alveolar bone area was determined as the combination of the trabecular bone area and bone marrow area in furcation. The level of the alveolar bone was determined by measuring the distance from the cemento-enamel junction to the alveolar bone crest (Figure 1C). Attachment level was measured as the distance between the cemento-enamel junction and the most coronal extent of connective tissue attachment to the cementum (Figure 1C). Alveolar bone and attachment level values were measured at the mesial and distal regions of the mandibular first molars. The means of all the measurements were used for data analysis.
Figure 1
(A) The measurement of the furcation area for histomorphometric analysis (H&E, 4×), (B) The measurement of alveolar bone area in furcation for histomorphometric analysis (H&E, 4×), (C) Histometric measurement of alveolar bone and attachment loss (H&E, 4×).
CEJ, cemento-enamel junction; CTA, connective tissue attachment; AC, alveolar crest.

The histomorphometric analysis was performed using a light microscope (BX50 research microscope, Olympus, Tokyo, Japan). Images were digitized with a camera (DP26 Digital Camera, Olympus, Tokyo, Japan) and analyzed with the OLYMPUS DP2-BSW application software by a calibrated examiner with no prior knowledge of the experimental design.
Intra-examiner reproducibility
Before histometric analyses were performed, the examiner measured 20 specimens twice with a one-week interval between measurements. Bland-Altman plots and intraclass correlation coefficients were used to evaluate the intra-examiner agreement and reliability [2223]. Bland–Altman plots display the agreement between the two values measured with a week interval for all histomorphometric parameters. The intraclass correlation coefficients (95% confidence interval) were 0.993 (0.982-0.997) for alveolar bone area measurements, 0.994 (0.986-0.998) for alveolar bone level measurements, and 0.993 (0.983-0.997) for attachment level measurements.
Quantification of MMPs and TIMP
Gingival tissues were removed from the alveolar bone, placed immediately in a sterile saline solution, and frozen at -80°C until biochemical analysis. In brief, before grinding, the tissue was blotted, weighed on a microbalance, and placed into a sufficient volume of phosphate-buffered saline (PBS; 4°C, pH 7.0) containing a protease inhibitor (5 μg/mL aprotinin, 1 mM EDTA) at a dilution of 10 mg tissue/mL PBS plus protease inhibitor solution. The samples were homogenized at 8,500 rpm for 30 seconds, four times at 10-second intervals, using a homogenizer (T25Ultra Turrax; Ika Labortechnik, Staufen, Germany). The homogenate was processed twice using freeze–thawing procedures and then sonicated three times with an ultrasonicator (SE Soniprep 150; Sanyo Gallenkamp, Leicestershire, UK) for 30 seconds, at 10-second intervals. The homogenate was centrifuged (Sigma 3K30, Osterode, Germany) at 15,000 rpm for 16 minutes, and supernatant was collected for MMP-1, MMP-8, and TIMP-2 analysis. The supernatant preparation processes were performed on frozen medium at 0–4°C. All samples were brought to room temperature for enzyme-linked immunosorbent assay. Gingival tissue concentrations were analyzed in each 300 µL sample (100 µL for each marker) by standard enzyme-linked immunosorbent assay apparatus at 450–550 nm using MMP-1 (E90097Ra; Uscn Life Science Inc., Wuhan, China), MMP-8 (E90103Ra; Uscn Life Science Inc.), and TIMP-2 (E90128Ra; Uscn Life Science Inc.) kits. The ratios of MMP-1 and -8 to TIMP-2 in the rat gingival tissues were also calculated. The samples that showed higher TIMP-2 concentrations were diluted (ten-fold) and measured in duplicate.
Statistical analysis
The data were tested for normality using the Kolmogorov–Smirnov test. One-way analysis of variance and Tukey’s post hoc test were carried out to compare histomorphometric data and MMP-1, MMP-8, and TIMP-2 levels between the groups after the normality of the data distribution had been checked. All tests were performed using SPSS software, version 19.0 (SPSS Inc., Chicago, IL, USA). P<0.05 was considered to be statistically significant.
RESULTS
Kaempferol was tolerated by all of the animals in the study, and the procedures were carried out appropriately, without complications.
Histomorphometric findings
Alveolar bone area (%) in the furcation region, alveolar bone level (µm), and attachment level (µm) values are summarized in Table 1. Significant increases in alveolar bone and attachment loss were observed in the experimental periodontitis group compared with the healthy control group (P<0.05), and the alveolar bone area was greater in the kaempferol application groups than in the control groups (P<0.05). The mean increases in alveolar bone area were 15.9% (kaempferol compared with saline in groups without ligature) and 22.8% (in groups with ligature) (P<0.05). Significant decreases in alveolar bone and attachment levels were observed in the kaempferol application groups compared with the control groups (P<0.05). The mean reductions in alveolar bone level were 6.1% (kaempferol compared with saline in groups without ligature) and 7.9% (in groups with ligature), and the mean reductions in attachment level were 16.0% (kaempferol compared with saline in groups without ligature) and 21.3% (in groups with ligature) (P<0.05). Histologic appearances are shown in Figure 2A-F.
Table 1
The percentage of alveolar bone in furcation area, alveolar bone level, and attachment level

Data are expressed as the mean ± standard deviation.
n=10 for each group.
One-way ANOVA and post-hoc Tukey's test.
CTRL, healthy control group; EXP PER, experimental periodontitis group; SLN, saline; KMP, kaempferol; Lig-, ligature was removed i15 days after ligature insertion; Lig+, ligature was kept in position during all experimental procedures.
a,b,c,d,e)Different letters represent statistically significant differences (P<0.05).
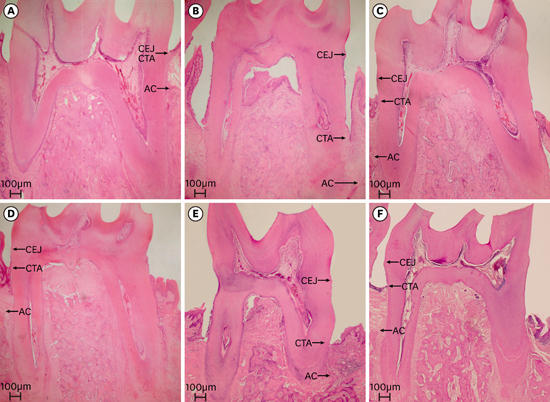
Figure 2
(A) The sections from the mesio-distal aspects throughout the mandibular first molars in CTRL (H&E, 4×), (B) The sections from the mesio-distal aspects throughout the mandibular first molars in EXP PER. (H&E, 4×), (C) The sections from the mesio-distal aspects throughout the mandibular first molars and the reference areas for histomorphometric analysis in SLN/Lig- (H&E, 4×), (D) The sections from the mesio-distal aspects throughout the mandibular first molars and the reference areas for histomorphometric analysis in KMP/Lig- (H&E, 4×), (E) The sections from the mesio-distal aspects throughout the mandibular first molars and the reference areas for histomorphometric analysis in SLN/Lig+ (H&E, 4×), (F) The sections from the mesio-distal aspects throughout the mandibular first molars and the reference areas for histomorphometric analysis in KMP/Lig+ (H&E, 4×).
CTRL, healthy control group; CEJ, cemento-enamel junction; CTA, connective tissue attachment; AC, alveolar crest; EXP PER, experimental periodontitis group; SLN, saline; Lig-, ligature was removed 15 days after ligature insertion; KMP, kaempferol; Lig+, ligature was kept in position during all experimental procedures.

Biochemical findings
Table 2 shows that MMP-1 and -8 levels were statistically higher in the experimental periodontitis group compared with the healthy control group (P<0.05). Gingival tissue MMP-1 and -8 levels decreased significantly in the kaempferol application groups compared with the control groups (P<0.05). The mean reductions in MMP-1 were 49.1% (kaempferol compared with saline in groups without ligature) and 61.5% (in groups with ligature), and the mean reductions in MMP-8 were 20.7% (kaempferol compared with saline in groups without ligature) and 28.0% (in groups with ligature) (P<0.05). MMP-1 and -8 levels were lower in the kaempferol application groups compared with the experimental periodontitis group (P<0.05). There were no statistically significant differences in TIMP-2 levels between the kaempferol and saline application groups (P>0.05). The mean differences in TIMP-2 were 26.8% (kaempferol compared with saline in groups without ligature) and 16.1% (in groups with ligature) (P>0.05). There were differences between the kaempferol application groups and the controls in terms of the MMP-1/TIMP-2 ratio (P<0.05), but there were no differences in the MMP-8/TIMP-2 ratio (P>0.05).
Table 2
Levels of MMP-1, MMP-8, and TIMP-2 in rat gingival tissues

Data are expressed as the mean ± standard deviation.
n=10 for each group.
One-way ANOVA and post-hoc Tukey's test.
CTRL, healthy control group; EXP PER, experimental periodontitis group; SLN, saline; KMP, kaempferol; Lig-, ligature was removed 15 days after ligature insertion; Lig+, ligature was kept in position during all experimental procedures.
a,b,c,d)Different letters represent statistically significant differences (P<0.05).
DISCUSSION
This study was designed to investigate effectiveness of the kaempferol application on the periodontium of rats using histomorphometric and biochemical analysis after experimental periodontitis induction with/without the presence of microbial dental biofilm. To the best of our knowledge, this is the first trial examining the effect of kaempferol application on periodontium by histomorphometric analysis and on gingival tissue MMP-1, MMP-8, and TIMP-2 levels by biochemical analysis in the experimental periodontitis model.
In this study, ligature-induced experimental periodontitis, a well-established model of experimental periodontitis in rats and a simple and reliable technique for disease induction, was used. Rat models are commonly used in experimental periodontitis studies because the structure and organization of the periodontal tissues are similar to those of humans [24]. The kaempferol dose (10 mg/kg every two days for ten days) was selected based on the study of Kim et al. [20], which reported that this dose confers anti-inflammatory effects without causing adverse effects.
MMP-1 and -8 belong to the interstitial collagenase group of the MMP family and serve as initiators of extracellular matrix destruction in rat tissues [9]. MMP-8 plays a more critical and major role in periodontal tissue destruction than MMP-1. However, MMP-1 rather than MMP-8 may affect the initiation of collagen destruction [25]. Kaempferol is a flavonoid found widely in dietary plants and commonly used in traditional medicine [17]. In many disease models, kaempferol has been shown to display a number of positive biological activities, such as antioxidant and anti-inflammatory effects [182627282930]. In the present study, it was shown that systemic kaempferol application significantly decreased gingival tissue MMP-1 and -8 levels during the two experimental periods. A direct comparison with other studies is not possible, as no other published studies to date have examined the effectiveness of kaempferol in periodontal disease. Nonetheless, our findings of significantly decreased levels of MMP-1 in the kaempferol application groups compared with the controls are in accordance with similar findings in various other studies [262728]. Kou et al. [26] found that kaempferol inhibits Porphyromonas gingivalis-induced mRNA expression of cyclooxygenase-2, IL-6, and -8, and MMP-1 and -3 in human gingival cells. It was also reported that kaempferol suppresses the expression of MMP-1 in rheumatoid arthritis synovial fibroblasts [27], and in two in vitro studies, it was found that kaempferol downregulated MMP-1 expression in human dermal fibroblasts [28]. In addition, Choi et al. [18] reported that kaempferol inhibits Prevotella intermedia lipopolysaccharide-induced production of nitric oxide in murine macrophages. According to these data, the authors documented that kaempferol can be used as a therapeutic agent in the treatment of periodontal disease [18]. Moreover, kaempferol inhibits monocyte chemotactic protein-1 gene expression and protein secretion in lipopolysaccharide-activated macrophages [29], and it prevents collagen breakdown by inhibiting collagenase in inflamed skin and photo-aged skin [30].
TIMP-2 inhibits all MMPs; however, it has a particularly strong inhibitory effect on MMP-8 [16]. Controversial results of TIMP-2 levels (lower [7], higher [11], and also absence of differences [31]) have been reported in periodontitis patients compared with healthy control subjects. MMP-8 and TIMP-2, which are found in higher levels in periodontitis patients, decrease after periodontal therapy [1115]. Marcaccini et al. [10] reported that MMP-8 levels were elevated during periodontal disease and lower after periodontal treatment, but there were no changes in TIMP-2 levels before and after periodontal therapy. Higher levels of MMP-1 were reported in periodontitis-affected gingival tissues compared with healthy gingival tissues, whereas TIMP-2 levels were similar in both groups. Moreover, the authors documented that MMP-1/TIMP-2 ratios were higher in periodontitis-affected gingival tissues than in the control tissues [31]. In the present study, TIMP-2 levels decreased after kaempferol application; however, the difference was not statistically significant when the kaempferol application and control groups were compared. In contrast to this finding, a previous study reported that kaempferol significantly reduced TIMP-2 mRNA expression and protein levels in oral cancer cells [32]. Similar to the findings of that in vitro study, Ginkgo biloba extract (mainly quercetin and kaempferol) downregulated the protein levels of TIMP-2 in rat mesangial cells [33]. It was also found that Ginkgo biloba reduced the expression of TIMP-2 in experimental diabetic nephropathy in rats [34].
MMP-1/TIMP-2 and MMP-8/TIMP-2 ratios were calculated in the present study, and it was found that the MMP-1/TIMP-2 ratio decreased in both kaempferol application groups. However, the MMP-8/TIMP-2 ratio was not significantly altered. Interestingly, the MMP levels were similar when the kaempferol application groups were compared, regardless of ligature status. The percentage reduction in MMPs between the kaempferol and control groups was also calculated. The mean reductions in MMP-1 were 49.1% (between groups without ligature) and 61.5% (between groups with ligature) and the mean reductions in MMP-8 were 20.7% (without ligature) and 28.0% (with ligature). No differences in MMP-8 levels were observed; however, MMP-1 reduction was significant. From the data presented in this study, it can be concluded that kaempferol application was more effective in inhibiting MMP-1 in the rats with ligature than in the rats without ligature.
In two experimental studies, it was found that in addition to its destructive properties, MMP-8 displayed protective and anti-inflammatory activity against Porphyromonas gingivalis-induced alveolar bone loss, which is inconsistent with the findings of the current study regarding MMP-8 [1213]. In considering the histomorphometric findings of the current study, the increased MMP-8 is probably related more to proinflammatory actions than to defensive processes, which is inconsistent with the two experimental studies.
Histological analysis is essential when evaluating periodontal regeneration and new treatment strategies [35]. The histomorphometric analysis performed in the present study demonstrated that the systemic application of kaempferol prevented ligature-induced alveolar bone loss and improved recovery of alveolar bone loss. The beneficial effect of kaempferol on the alveolar bone in the furcation area was observed after experimental periodontitis induction with/without the presence of microbial dental biofilm. In the present study, not only alveolar bone but also soft tissue was positively affected by kaempferol application during the two periods. The positive effects on alveolar bone might originate from several underlying mechanisms, including (1) inhibition of receptor activator of nuclear factor kappa-B ligand-induced osteoclast differentiation [36]; (2) stimulation of osteoblast differentiation [37]; (3) activation of bone morphogenic protein signaling [38]; (4) blockage of estrogen receptors [39]; (5) inhibition of reactive oxygen species production [18]; and (6) stimulation of bone sialoprotein gene transcription [40]. From a clinician’s perspective, it is worth noting that kaempferol-rich diets or drugs including kaempferol might help in the clinical management of periodontal disease.
The potential limitations of our study are the lack of host-modulating drug groups (e.g. subantimicrobial dose doxycycline as adjunctive treatment for periodontitis) and additional biomarkers (such as MMP-9, TIMP-1) and the effect on other tissues and organs. These factors could be important in understanding the role of kaempferol in periodontitis as a treatment strategy. In the present study, however, the question that was investigated was whether kaempferol could play a beneficial role in inflammatory response. Taken together, the results of this study suggest that kaempferol has some positive effects on the periodontium and that it may be used as a drug to modulate host response in periodontitis.
This study showed that systemic kaempferol application reduced MMP-1 and -8 levels and improved hard (increasing alveolar bone area in furcation and decreasing alveolar bone loss) and soft (coronal displacement of connective tissue attachment) tissue healing in a ligature-induced experimental periodontitis model. However, no effect on TIMP-2 levels was observed.
The results suggest that kaempferol application might be a valuable treatment alternative for preventing alveolar bone resorption and attachment level. Considering the histomorphometric and biochemical findings, kaempferol might help as a potential host modulating agent in developing new therapeutic strategies for treating periodontal disease. In terms of clinical importance, individuals with periodontitis can be advised to eat foods that contain kaempferol to support periodontal disease treatment. Further studies are needed for a complete evaluation of the merits and side effects of kaempferol, as well as to confirm these important findings on different modulator agent groups with other biomarkers related to periodontal pathogenesis.
 XML Download
XML Download