

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
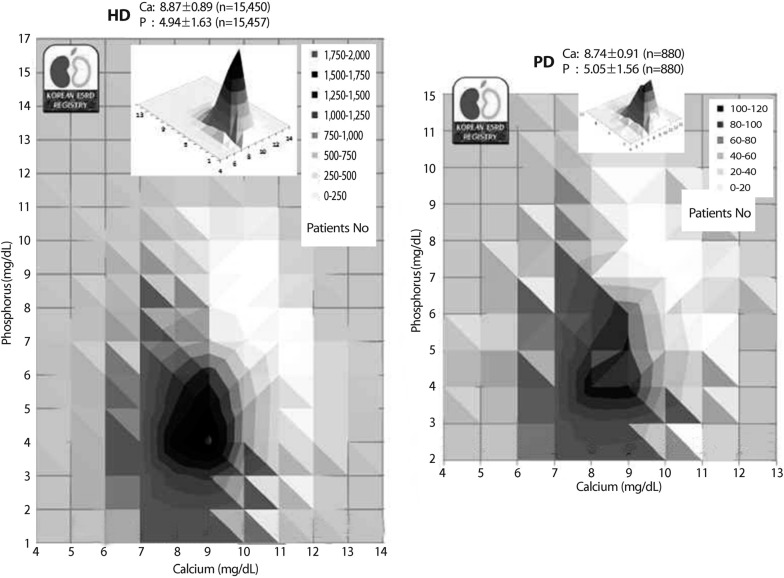
The Korean Society of Nephrology has maintained an end-stage renal disease (ESRD) registry since 1986. However, serum mineral data have only been collected since 2012. In 2013, there were 59,918 dialysis patients registered by the Korean Society of Nephrology (hemodialysis, 52,378; peritoneal dialysis, 7,540). Mean serum phosphorus levels were 4.94±1.63 and 5.05±1.56mg/dL in patients with hemodialysis (n=15,457) and peritoneal dialysis (n=880), respectively. Serum calcium concentrations were 8.87±0.89 and 8.74±0.91mg/dL in hemodialysis (n=15,450) and peritoneal dialysis (n=880), respectively. The mean values of calcium and phosphorus appear acceptable in both hemodialysis and peritoneal dialysis patients, but the standard deviations, especially of phosphorus, were quite large1) (Fig. 1).
The term 'chronic kidney disease-mineral bone disorders' (CKD-MBD) is a new term that, in contrast to the old term 'renal osteodystrophy', implies a systemic syndrome associated with cardiovascular morbidity and mortality2). Previous studies have shown that elevated serum calcium, phosphorus, and parathyroid hormone (PTH) levels are associated with increased cardiovascular mortality as well as all-cause mortality3). In order to improve outcomes in patients with CKD-MBD, many countries have developed clinical practice guidelines. Globally, the Kidney Disease Outcome Quality Initiative (KDOQI) and Kidney Disease: Improving Global Outcomes (KDIGO) guidelines are the most commonly used4,5). However, whether those global guidelines can be successfully implemented at the local level remains to be examined. As a regional guide, the Japanese Society for Dialysis Therapy (JSDT) recently updated its clinical practice guidelines for the management of CKD-MBD6).
Serum mineral targets in KDOQI and KDIGO guidelines
In CKD stages 5 and 5D, the KDOQI (2003) guidelines recommend that serum phosphorus be maintained at 3.5-5.5mg/dL4). This target corresponds to a level slightly higher than the normal reference limit. The KDIGO(2009) guidelines suggest lowering phosphorus levels toward the reference range in CKD stage 5D5). Notably, both guidelines had low levels of evidence supporting this guideline.
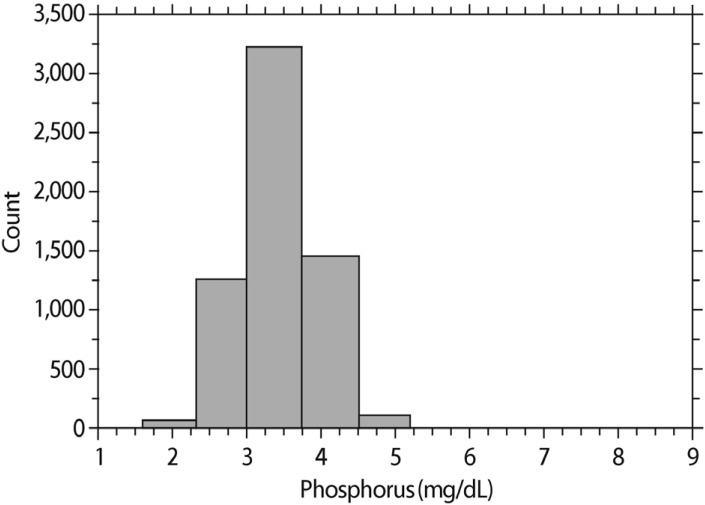
According to Western textbooks, normal serum phosphorus ranges from 2.5 to 4.5mg/dL7). In this study we sought to determine if these guidelines could be applied to Korean patients. Excluding those who had an estimated glomerular filtration rate (eGFR) <60mL/min/1.73m2 calculated by Modification of Diet in Renal Disease (MDRD) equation, we analyzed serum phosphorus concentrations from 6,131 adults (male 3,163; female 2,968) participating in a health check-up at our hospital in 2011. The mean age and eGFR were 45±11 years and 92±14 mL/min/1.73m2, respectively. The serum phosphorus distribution is shown in Fig. 2. Based on the mean and standard deviation data, the normal serum phosphorus concentration in this patient population ranged from 2.4 to 4.5 mg/dL. This data indicates there are no differences in the normal levels of serum phosphorus between Korean and Western patients. In the United States, a high serum phosphorus concentration was associated with a low socioeconomic status irrespective of race8).
The KDOQI (2003) guidelines recommend that serum corrected calcium be maintained at 8.4-9.5mg/dL in CKD stages 5 and 5D4). This range corresponds to the lower end of the reference range. The KDIGO(2009) guidelines suggested maintaining serum calcium levels in the reference range in CKD stages 3 - 5D5). The Ca×P product was previously considered an important biomarker9), and the KDOQI (2003) guidelines recommended Ca×P be <55mg2/dL2. However, individual serum calcium and phosphorus values are currently used as the primary determinants for target serum ranges.
Hemodialysis quality monitoring by HIRAS in Korea
In Korea, the national government or Health Insurance Review and Assessment Service (HIRAS) assesses hemodialysis quality on an annual basis. Every hemodialysis facility should test serum phosphorus and calcium monthly in all patients. From this data, the Ca×P product is calculated and evaluated as an outcome variable, and HIRAS requires the product to be below 55mg2/dL2, consistent with the KDOQI guidelines. The value of Ca×P product is currently an important criterion for the assessment of national health insurance coverage in Korea when calcium-free phosphate binders are prescribed.
Gaps between global guidelines and local practices for management of CKD-MBD
A few years ago, serum mineral data were collected from 1,018 maintenance hemodialysis patients at 17 centers in Korea10). When classified by the ranges recommended by the KDOQI guidelines, only about half of the patients were considered within the guideline range for serum Ca and P. Uncontrolled hyperphosphatemia and a Ca×P product greater than or equal to 55mg2/dL2 were noted in about 40% and 30% of patients, respectively. Approximately 30% of patients were within the guideline range for PTH, with a greater proportion of patients falling in the lower PTH range, revealing a gap between guidelines and practice.
Our data were similar to those from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Although there were some differences between countries, approximately half of the patients had uncontrolled hyperphosphatemia >5.5mg/dL. It is notable that almost every country showed that phosphorus tended to decrease slowly over the study period. On the other hand, PTH levels were steady throughout the 3 phases of DOPPS. About half of the patients appeared to have PTH levels within the target range 11).
A regional, but not global, guide from Japan
Patients in different countries are affected by different medical and social circumstances12). The Japanese CKD-MBD guidelines were updated last year and had an impact on the care of Korean dialysis patients. They proposed a simplified diagram illustrating what medications can be adjusted according to serum phosphorus and corrected calcium levels, in which the serum phosphorus target was 3.5 to 6.0mg/dL6).
In the Japanese epidemiological data from hemodialysis patients, those with serum phosphorus near 5mg/dL, calcium near 9mg/dL, and PTH near 180 pg/mL showed the best survival rate13). Based on these results, the Japanese guidelines suggest higher target levels of serum phosphorus (6mg/dL) and calcium(10mg/dL), respectively6).
Gaps between guidelines
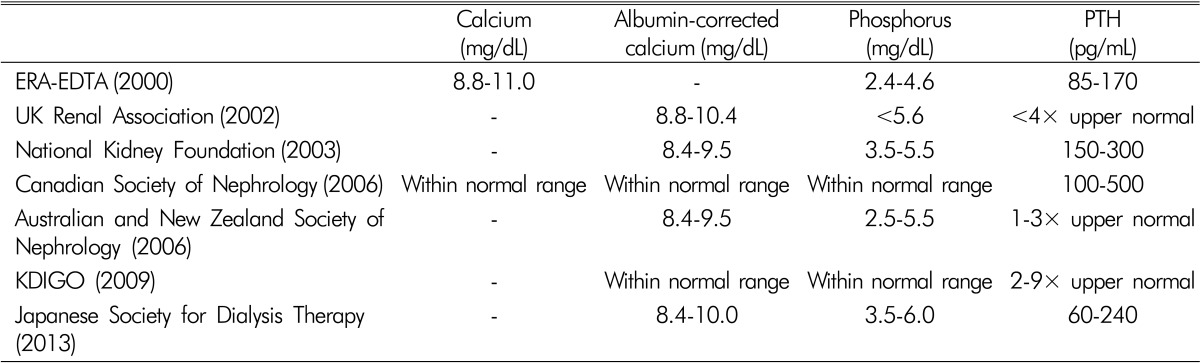
Table 1 summarizes the recommended serum phosphorus, corrected calcium, and PTH levels in patients undergoing dialysis according to different professional organizations. As shown in the table, differences exist among the international guidelines. Although KDIGO is updating CKD-MBD guidelines through Controversies Conferences 14), the serum mineral targets will not be changed until data from randomized controlled clinical trials supports such changes.
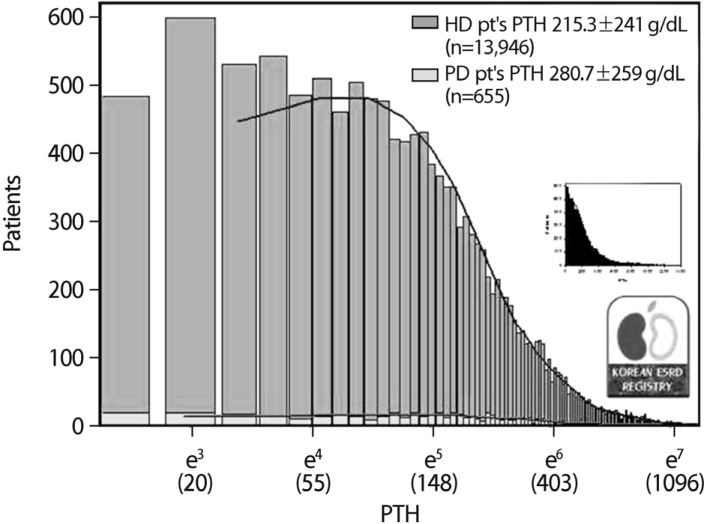
Many nephrologists around the world use these guidelines when they manage patients with CKD-MBD. Accordingly, more hemodialysis facilities in the United States adopted a high PTH target after the KDIGO guidelines were introduced15), and the serum calcium target subsequently increased. The serum phosphorus target did not change, and most facilities currently adhere to a target level of 5.5mg/dL. In contrast to the upward trend of PTH target in the United States, many Korean dialysis patients have low PTH levels1), and approximately 20% of the patients were medicated with vitamin D receptor agonists or cinacalcet (Fig. 3).
In our study population, the utility of the Japanese PTH target range is appreciated. PTH levels were proposed to range from 60 to 240 pg/mL6) based upon the odds ratios for achieving the Japanese calcium and phosphorus targets13). The underlying idea was that appropriate PTH regulation could be maintained by optimal control of serum phosphorus and calcium levels.
Relative importance of hyperphosphatemia control
The Japanese hemodialysis cohort study evaluated the relative importance of calcium, phosphorus, and PTH control13). Patient survival was higher when phosphorus was well controlled as compared with calcium and PTH. PTH had a weak influence upon mortality compared with phosphorus and calcium.
We found that, in our hemodialysis population, PTH levels were significantly associated with phosphorus and calcium levels10). In patients with a high PTH level, both phosphorus and calcium were poorly controlled.
Conclusion
There are gaps between global guidelines and local practices. Many dialysis patients are not within the recommended range of serum phosphorus, calcium, and PTH. Among the 3 mineral values, serum phosphorus may be most influential on mortality outcomes. However, global or international CKD-MBD practice guidelines suggest different target levels for serum phosphorus. The serum phosphorus target associated with the best outcomes should be determined for each local area, and further study on Korean populations is needed to support dialysis management guidelines.
 XML Download
XML Download