

 PDF
PDF ePub
ePub Citation
Citation Print
Print


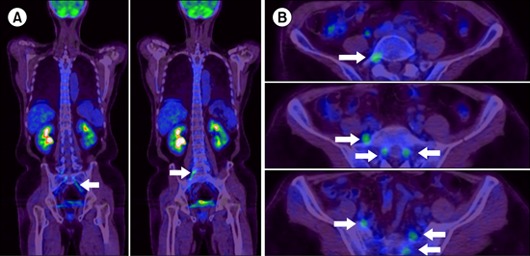
A 53-year-old man with a history of diabetes presented with weakness in both legs accompanied by numbness and pain. Eight months previously, he had a pelvic mass that caused pain during defecation and was diagnosed as having diffuse large B cell lymphoma. He received 6 cycles of R-CHOP chemotherapy and field radiation therapy (dose, 44 Gy). No hypermetabolic lesions were detected by positron emission tomography (PET)-computed tomography scanning. Two months later, he presented with the above neurological manifestations, including right facial palsy. Brain and spine magnetic resonance imaging did not find any evidence of lymphoma involvement. A cerebrospinal fluid (CSF) cytological study was also negative. A nerve conduction study showed delayed peak latencies and reduced amplitudes of sensory nerve action potentials in both the sural nerves. Reduced amplitude of combined motor action potential and conduction velocities were identified in both the deep peroneal nerves. The patient had a history of diabetes and hepatitis C, but because of sensorimotor nerve involvement, polyneuropathy associated with underlying systemic disease or chemotherapy toxicity was not diagnosed. Sequential 18F-fluoro-2-deoxy-D-glucose (FDG) PET images showed increased 18F-FDG uptake (SUVmax, 4.11) along the bilateral lumbosacral plexus (arrow). A second CSF study revealed malignant lymphoma cells (A, B).
 XML Download
XML Download